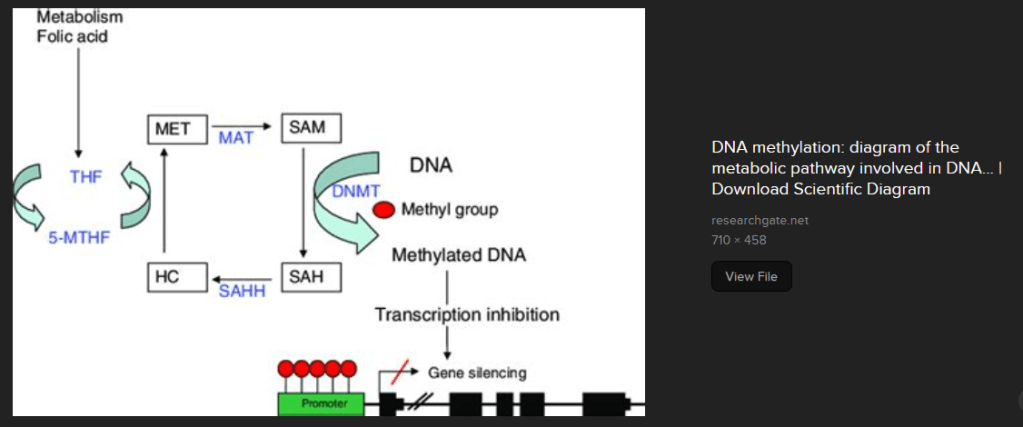
Adenosyl homocyteinase is a methyl group transferring enzyme that is inhabited by copper in the +2 oxidation state. We were trying to better understand the process of gene silencing by methylation, see below. In the process we discovered the mechanism of how +2 oxidation state copper might be bad for our hearts.
Some UniProt.org highlights
UniProt.org is a site scientists consult to learn more about proteins. This is where it was discovered that
Adenosylhomocysteinase (SAHH protein, ACHY gene) catalyzes the hydrolysis of S-adenosyl-L-homocysteine to form adenosine and homocysteine. Hydrolysis is the use of a water molecule (H2O) to cleave the first molecule into two new molecules. One molecule gets an “H” and the other gets an “OH.” According to the AI written UniProt blog SAH binds copper ions (By similarity). NAD+ is also a cofactor. The copper part of the story deserves some followup by a PubMed search or simply going to the PubMed that the AI program left us with.
Note that this reaction can go in both directions. H2O can be used to cut S0adenosyl-L-homoclyteine or it can be liberated by “fusing” L-homocysteine with adenosine.
This is the reference to the actual scientific study.
Li M, Li Y, Chen J, Wei W, Pan X, Liu J, Liu Q, Leu W, Zhang L, Yang X, Lu J, Wang K. Copper ions inhibit S-adenosylhomocysteine hydrolase by causing dissociation of NAD+ cofactor. Biochemistry. 2007 Oct 16;46(41):11451-8. PubMed
This study demonstrated that Cu2+ bound to SAHH and decreased its affinity for cofactor NAD+.
Back to the SAHH products and reactants
Things are tricky here because our Cu(II) inhbited wenzyme SAHH can go in both directions. Many readers may recognize the products/reactants as substances used in diagnostic blood tests.
Adenosine acts on receptors in our blood vessels that might increase blood flow. It is also used in medical tests of our heart function. According to the Cleveland clinic homocysteine can indicate an increased risk for cardiovascular disease. According the Health Matters S-adenosylhomocysteine is also used as a risk factor for cardiovascular disease. Health Matters references peer reviewed publications stating that S-adenosylhomosysteine may be a more sensitive marker than homosysteine because the former can inhibit DNA methylation enzymes that turn genes off. DNA methylation can turn good genes off too.
SAHH and turning genes off.
This post is not going to explore the scientific study related to this image. Putting methyl groups on the promoter of a gene prevents the gene from being transcribed into messenger RNA that gets translated to protein by our ribosomes. While we know that Cu(II) inhibits one enzyme , SAHH, in this process, we do not know what the impact, if any, of consuming Cu(II) will have on DNA methylation.
This post is not meant to say that taking a Cu(II) will inhibit this cycle. If one is to take a copper supplement maybe, just maybe,a Cu(I) might be better.
We found an absolutely beautiful image of cytochrome C oxidase activity in a skeletal muscle section. [1] This site failed to reference the claim that 3% of the muscle fibers in the elderly are deficient in the copper cofactor enzyme cytochrome C oxidase (CCO) enzyme activity. CCO/complex IV terminates the electron transport chain of the mitochondria. Naturally this claim had to be investigated. An internet search was performed for more beautiful images of CCO activity in aged human muscle sections.
We found an excellent 2011 publication that investigated the increased age related muscle frailty in AIDS patients on long term retroviral treatment. [2] This paper had much to say about the retrovirals accelerating the accumulation of mutations in the mitochondria genome which contains the gene for CCO. A keyword search of the PDF file of this paper for “copper” revealed nothing!
This year, 2023, an amazing review was published in Experimental Gerentology on muscle aging. [3] “Ultrastructural changes, including loss of type I and type II myofibers and a greater proportion of cytochrome c oxidase deficient” was a major theme, but not one word whatsoever on copper! What? This cannot be!
Then we found a 2003 paper on the use of copper deficiency to accelerate cardiac muscle aging in a rat model was discovered that explains so much. [4] This research was performed before 2004 when 90% of the human genome had been sequenced. [5] Technology has enabled us to learn so much more, yet we are forgetting the basics. A brief nod may be given to a new 2018 assay to measure CCO activity deficiency in small tissue samples.[6]
Never mind genes, diet induced CCO deficiency and more
Ten weaning rats were fed a casein based diet that was copper adequate diet and allowed to eat as much as they pleased. Another ten had a casein based copper deficient diet and were also allowed to eat as much as they pleased.
The food that these rats was recorded. Then another two groups of ten rats were fed 80% of the rats that were eating as much as they liked. copper-adequate diet (5.0 μg Cu/ g diet) or copper-deficient diet (0.3μCu/g diet) for five weeks after which time their hearts were harvested. Two different different observations were being pursued with this study.
Copper deficiency causes mitochondrial oxidative stress by depriving cytochrome C oxidase of adequate copper.
Caloric restriction is a good thing.
Over the course of this study the rats grew from about 78 g to about 200 to 270g. The rats eating as much as they wanted of the copper adequate grew significantly more than the other three groups. Food restricted/ copper adequate rats experienced the same growth as the copper deficient rats that were allowed to eat as much as they wanted. Food restricted, copper deficient rats grew significantly less than the other three groups. There was no statistical synergy between copper deficiency and food restriction. The 10% adequate copper in the diet meant about 10% control copper in the liver. Copper deficiency tended to decrease the amount of iron sticking around in the liver.
Multifaceted mitochondrial issues with copper deficiency
Before looking at important “and more” enzymes other than cytochrome C oxidase in complex IV, we need a cartoon.
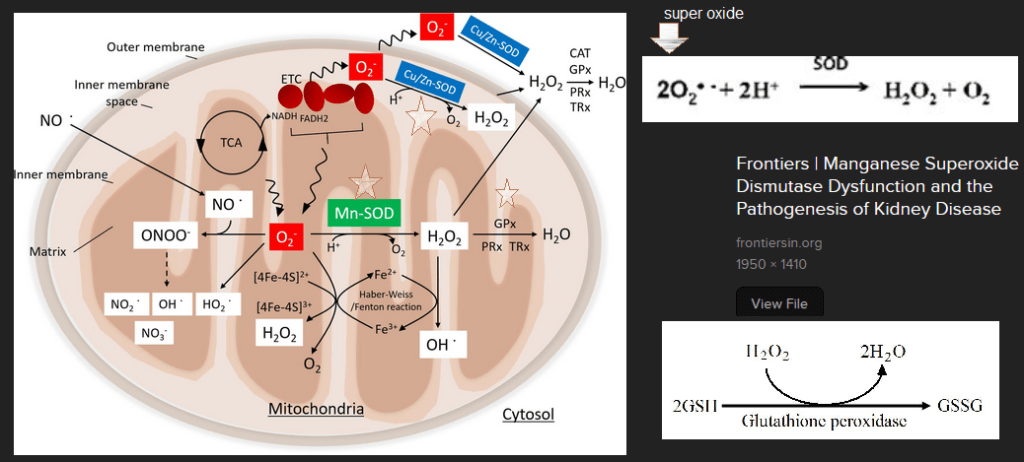
This image came from Looking for Diagnosis which does an excellent job of explaining genetic cytochrome C oxidase deficiency.
The Looking for Diagnosis does an excellent and quick overview of how mutations in proteins involved in getting Cu to complex IV can cause production of reactive oxygen species. (ROS). Note the decrease in glutathione peroxidase activity as well as the minochondria’s resident scavenger of superoxide O2– Manganese superoxide dismuase, also called SOD2. Note the one O2 picking up one electron e–. This is a math mistake. The cartoon should have two yellow circle electrons taking O2 to H2O. When our bodies make the same mistake we reduce O2 to the deadly reactive oxygen species super oxide written as O2â—- The “â—” is chemistry for a an unpaired electron. Electrons in this life are always looking to pair up.
One of them is blood vessel relaxing nitric oxide (NO) to from reactive nitrogen species peroxy nitrite ONOO–
Role of superoxide dismutases and glutathione peroxidase
Then we get to our dynamic dual. Both starred superoxide dismutases (SOD) take superoxide back to oxygen and hydrogen peroxide, H2O2.
Glutathione peroxidase takes reduced glutathione (GSH) and H2O2 and gives us harmless H2O and oxidized GSSG.
The Mitochondria cartoon with key enzymes MnSOD, GPx, and Cu/Zn SOD starred was obtained with an Internet search and a screen capture of the scientific article that went into details. Other screen captures of the reactions carried out by these enzymes have been added.
Now that we know the dynamic dual, let’s look at data
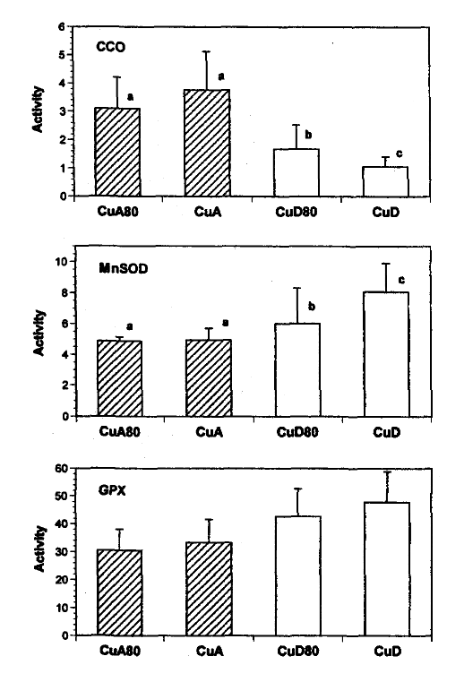
Figure 1: Activities of cytochrome c oxidase (CCO), manganese superoxide dismutase (MnSOD) and glutathione peroxidase (GPX) in mitochondria isolated from the hearts of rats fed copper-adequate diet either ad libitum (CuA) or at 80% of the ad libitum intake (CuA80) and copper-deficient diet either ad libitum (CUD) or at 80% of the ad Ubitum intake (CUD80). Enzyme activities are expressed as Units/mg protein. Values shown are means±SD.
where a unit of CCO is the amount that catalyzes the oxidation of μmol ferrocytochrome c / min, For non chemists, they are looking at color changes in ferrocytochrome C per minute.
a unit of MnSOD is the amount that causes 50% inhibition in the rate of pyrogallol autoxidation, Superoxide likes to react with pyrogallo causing a color change.
and a unit of GPX is the amount that catalyzes the oxidation 1 nmol NADPH / min.
The authors did some math so that they could meet the rule requirement to use a statistical technique called the 2-way ANOVA.
enzyme
diet
food restriction
combination of the two
CCO
P=0.0001 99.999% sure
P=0.067 93.3% sure
P=0.0002 99.998% sure
MnSOD
P=0.0006 99.994% sure
P=0.01 99% sure
P=0.01 99% sure
GPx
P=0.0001 99.999% sure
P=0.14 86% sure
P=0.052 94.8% sure
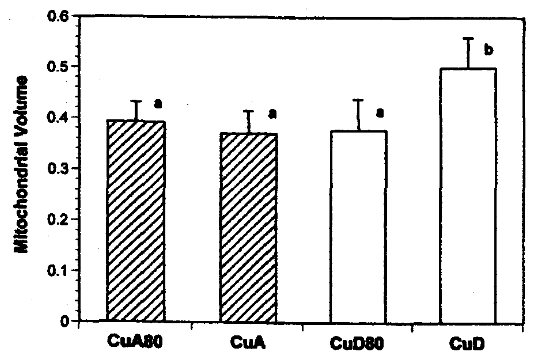
volume of mitochondria
P=0.008 99.2% sure
P=0.002 99.8% sure
P=0.0001 99.99% sure
P values from the figure legends have been translated into % certainty that the observed changes are not due to random chance. 95% certainty is generally considered the cutoff.
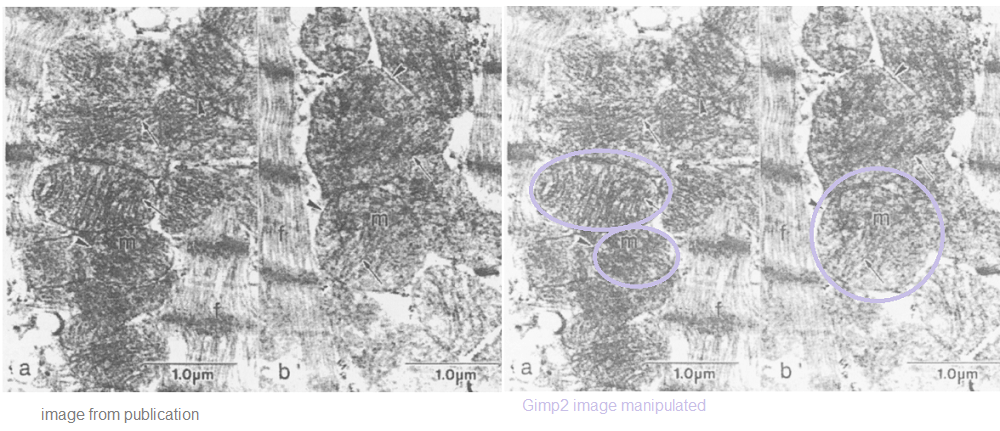
Even back in 2004 mitochondria swelling was a common symptom of copper deficiency. These are two images of heart cross sections analyzed by electron microscopy. The image on the right was adjusted in a free version of PhotoShop called Gimp2.
Electron micrographs of mitochondria (m) from hearts of rats fed copper-adequate (panel a) or copper-deficient (panel b) diets ad libitum. The myofibrillar component is indicated (f). The general morphology of the mitochondria, the outer membranes(arrowheads) and the cristae (arrows) demonstrate no detrimental effects associated with the copper-deficient diet.
FIGURE 4: Mitochondrial size in hearts from rats fed copper-adequate diet either ad libitum (CuA) or at 80% of the ad libitum intake (CuA80) and copper-deficient diet either ad libitum (CUD) or at 80% of the ad libitum intake (CUD80). Mitochondrial volumes are relative to myocardium minus nuclear volume.
What does this mean for humans?
The take home is that a diet deficient in copper for five weeks really decreased cytochrome C oxidase activity as well as activity of anti-oxidant enzymes MnSOD and GPx. The authors didn’t even analyze for Cu/Zn SOD! Johnson and Newman [4] also did not measure copper content in the rats’ hearts. [4] The odd thing is that of the rats with unrestricted food access the final weight was~270 vs ~240 g. How do we know we are getting enough copper? Five years ago an assay was published to detect cytochrome C oxidase activity in muscle (not heart) biopsies of rodents and humans. [6] Dr Leslie Klevay, also of the University of North Dakota, has spent his career studying copper deficiency. Here is a direct quote from a 2022 review’s conclusion. [7]
“One can conclude from numerous medical articles that copper deficiency contributes to, and probably causes, Alzheimer’s disease, ischaemic heart disease, some myelodysplastic syndrome and postmenopausal osteoporosis. These chronic diseases have low organ copper and impaired metabolic pathways dependent on copper. They improve with supplements containing copper. Thus, they exhibit classical characteristics of deficiency.” [7]
The study of Johnson and Newman [4] gives us some onsite on the what might be the cause of multi-organ disease states: loss of cytochrome C oxidase activity and anti-oxidant helpers MnSOD and GPx. [4]
Payne BA, Wilson IJ, Hateley CA, Horvath R, Santibanez-Koref M, Samuels DC, Price DA, Chinnery PF. Mitochondrial aging is accelerated by anti-retroviral therapy through the clonal expansion of mtDNA mutations. Nat Genet. 2011 Jun 26;43(8):806-10. PMC free article
Picca A, Lozanoska-Ochser B, Calvani R, Coelho-Júnior HJ, Leewenburgh C, Marzetti E. Inflammatory, mitochondrial, and senescence-related markers: Underlying biological pathways of muscle aging and new therapeutic targets. Exp Gerontol. 2023 Jul;178:112204. PMC free article
Johnson WT, Newman SM Jr. Copper deficiency: A potential model for determining the role of mitochondria in cardiac aging. J Am Aging Assoc. 2003 Jan;26(1-2):19-28. PMC free article
Simard ML, Mourier A, Greaves LC, Taylor RW, Stewart JB. A novel histochemistry assay to assess and quantify focal cytochrome c oxidase deficiency. J Pathol. 2018 Jul;245(3):311-323. PMC free article
Klevay LM. The contemporaneous epidemic of chronic, copper deficiency. J Nutr Sci. 2022 Oct 11;11:e89. PMC free article
What is new (to us) for Cu(I) in cardiovascular disease
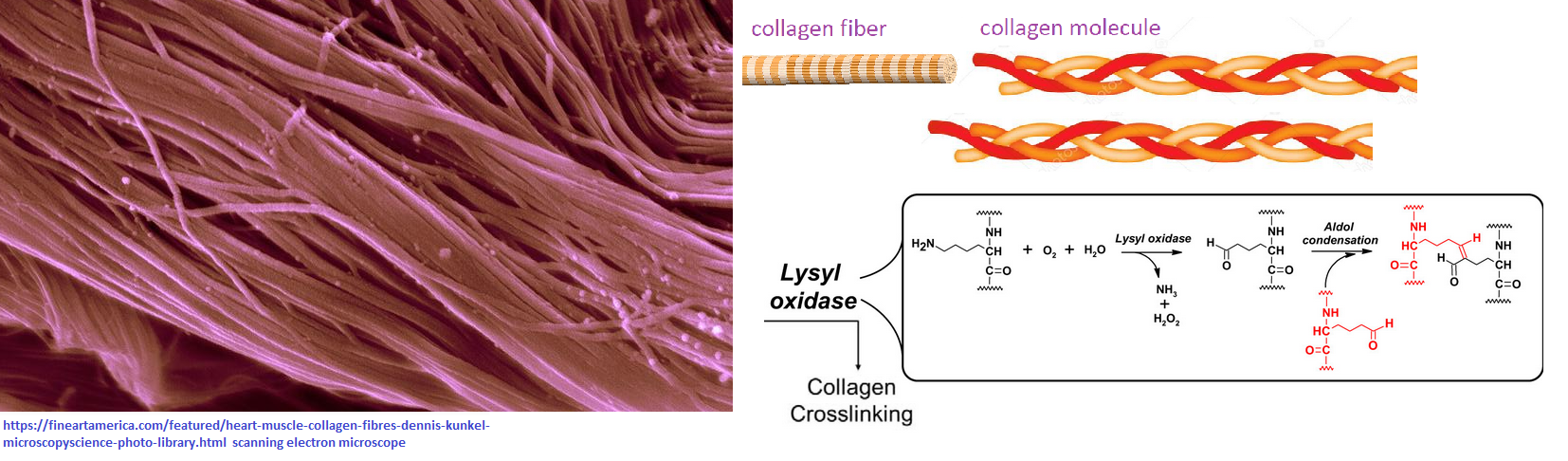
We at CopperOne have been obsessed with Covid. In the process of honoring our late colleague George Brewer, we are reexamining the Cu(I) literature. In 1973 Leslie Klevay was perhaps first to sound the alarm that a high ratio of zinc to copper in the drinking of rats fed egg white protein, sucrose, and vegetable oil could raise cholesterol and contribute to heart disease. [1] Eight years later Klevay and Viestenze published a report that rats on a copper deficient diet had abnormal electrocardiograms as well as a 39% increase in blood cholesterol. [2] It’s been close to 50 years since Dr Klevay’s first report. What have we learned? What we are learning is that maybe the copper dependent collagen cofactor enzyme lysyl oxidase may be an important player that is being overlooked. Lay readers might want to skip to the end for a cartoon summary of our journey through the literature.
Three reviews, back up of animal data
We have posted much on copper handling proteins on this website. What do experts in heart disease say in their reviews on copper? More importantly, what do the latest animals studies say on copper deficiency and heart disease?
Who authored these reviews?
[3] James J DiNicolantonio is part of the Mid America Heart Institute and author of The Salt Fix. Dennis Mangan is a sales and scientific communication guy. James H O’Keefe is a scientist at CardioTabs, a dietary supplement company, and on the staff at the Mid America Heart Institute.
[4] Tohru Fukai and Musuko Ushio-Fukai are affiliated with the Vascular Biology Center at the Medical College of Georgia in Augusta. Jack Kaplan is in the Department of Biochemistry and Medical Genetics at the University of Illinois, Chicago
[5] Yun Liu is part of Guangzhou Medical University in China. Ji Miao is now at Boston Childrens. Dr Miao studies copper deficiency in a number of rodent models of human diseases.
back up Cu deficient animal studies
Roberto Olivares is a professor at the Universidad de Buenos Aires. Cattle were made Cu deficient with a diet supplemented with sodium molybdate (11 mg of Mo/kg). The other group received 9 mg/kg copper sulfate. Each group and nine bovine that were followed for close to a year. [6] After almost a year Cu deficiency had no significant influence on weight but halved the serum Cu and decreased the heapatic Cu to less than 5% of the control. [6]
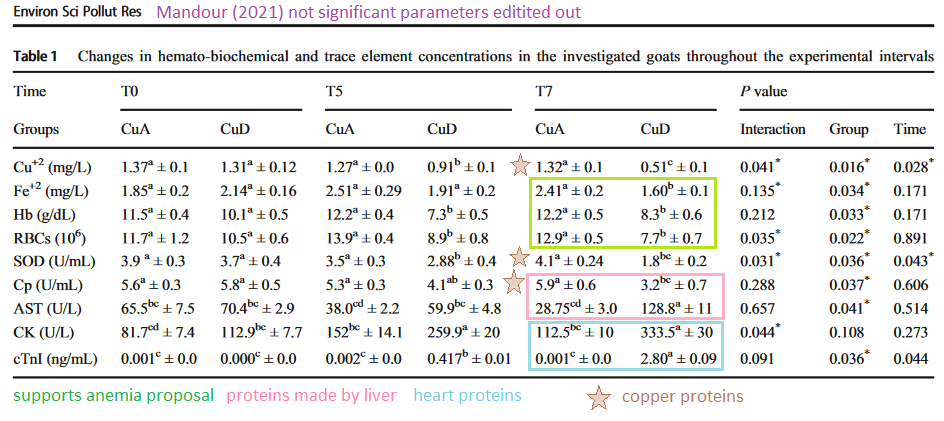
Ahmed Mandour of Suez Canal University and other authors from Egypt and Japan compared cardiovascular measurements of copper adequate and deficient goats. [7] Male Shiba goats were fed a diet of alfalfa hay cubes supplemented with 11 mg of Cu+2/kg dry matter. Molybdate sulfate was used to induce Cu deficiency. [7] These animals were followed for seven months with electrocardiograms, echocardiograms, and routine blood work. [7]
Ctr1
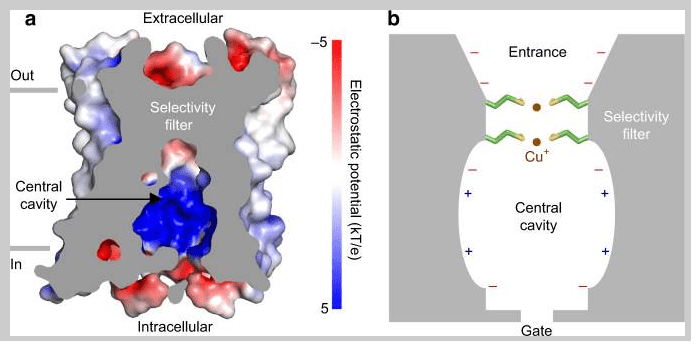
The DiNicolantonio review did notCtr1. [3] The Fukai gave a good discussion of structural components in transporting Cu+ [4]. The Liu/Miao review alsocovered the need for prior reduction of Cu2+ to Cu+, perhaps by STEAP, for transport by Ctr1 [4,5] The Liu/Miao review also discussed the consequence of Ctr1 down down in rodent heart disease models. [5]
Figure 3, from Ren (2019). A charge on the interior of Ctr1 b. a cartoon version of the entrance, selectivity, filter, and central cavity.
We’ve discussed this image on our own Ctr1 post. Personal communications with Ji Miao reiterate our conviction that Cu+ is most natural and least toxic way to absorb copper.
atox
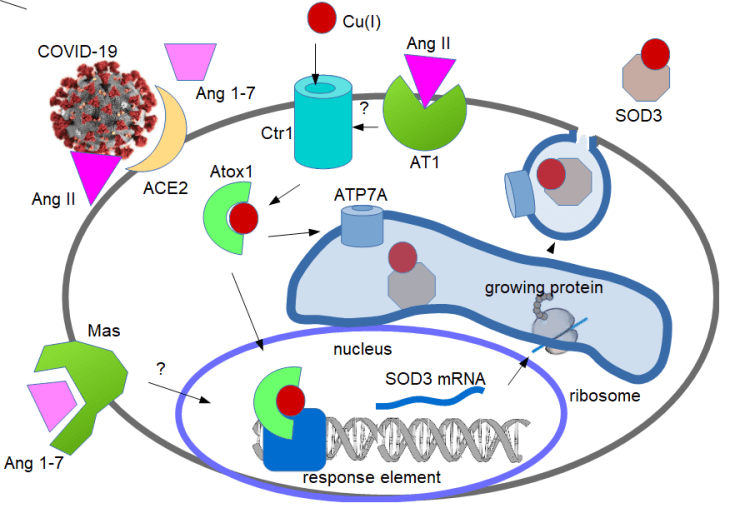
The Fukai review mentioned the anti oxidant protein 1 (Atox1) being both a chaperone ferry from the Ctr1 to the nucleus as a transcription factor [4] The Liu/Miao review discussed the interplay between Atox1, angiotensin II, and expression of Cu/Zn SOD3. [5] We’ve discussed this in another post on Atox1 in Covid… of course.
Copper in the +1 oxidation is involved in several levels in producing Cu/Zn SOD3 (1) as acquired by Cu(I) channel Ctr1 (2 ) in chaperone/transcription factor Atox1, (4) in channel ATP7A that loads Cu in Golgi where SOD3 is being processed for secretion.
Atox1 in Covid post went into more details into the cardiovascular function of angiotensin II in increasing blood pressure and how Cu/Zn SOD3 mitigates this response.
Other chaperones
We have covered copper chaperones in another post. The DiNicolantonio review had very little to say about chaperones, but much to say about SOD. [3] Not yet covered on this site is the production of peroxy nitrite when NO reacts with nitric oxide. NO. is needed to relax blood vessels. The Liu/Miao review makes brief mention of SCO1-2, the cytochrome C oxidase assembly protein, and mutations that can cause heart disease [5]. The Fukai review mentioned SCO and went into more detail about CCS, the chaperone for Cu/Zn SOD. [4]
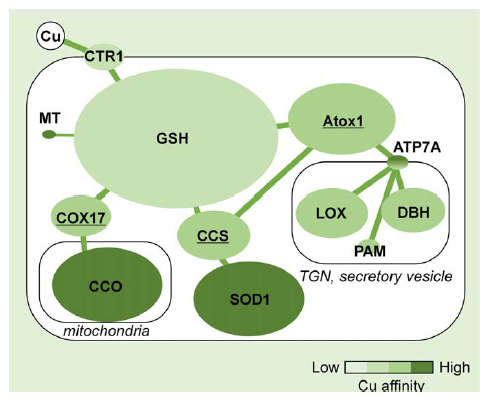
From Hatori, 2017 [18]
GSH chaperone of Cu+was covered in another post. The affinity of GSH complexes for Cu may not be as it was pictured in the Hatorie review covered on the copper chaperones post. We have largely ignored PAM, peptidylglycine alpha-amidating monooxygenase. Dopamine beta hyroxylase (DBH) is also largely off the radar in terms of cardiovascular disease reviews. What are the important copper cofactor enzymes in heart disease?
Cu/Zn SOD
All reviews agree that the ability of Cu/Zn superoxide dismutase to scavenge superoxide is important. [3-5] In the bovine study, cardiac Cu/Zn SOD activity decreased from 23.8 ± 7.2 to 16 ± 5.4 U per gram tissue in the Cu adequate versus deficient animals. [6] Thiobarbituric acid reactive substances (TBARS) are formed as a byproduct of lipid peroxidation. These were increased from 76.9 ± 27.2 to 154.3 ± 37.4 moles per gram heart in the Cu adequate versus deficient bovines. [6]
Table 1 from Mandour 2021 Values are expressed as mean ± SEM (n = 4). Hematological and biochemical parameters in copper adequate (CuA) and copper-deficient (CuD)groups analyzed using two-way ANOVA. The lowercase letters are fitted for comparing means between groups. LSD < 0.05. * P < 0.05 fitted to compare the significance of group, time, and interaction. These are blood values. Cardiac TnI is a blood marker for cardiac injury. Comments are those of CopperOne.
By the seventh month, the copper deficient goats had a notable decrease in SOD activity and ceruloplasmin ferrioxidase activity. Cardiac troponin I is a heart protein that only appears in the blood when the heart has been damaged. Ceruloplasmin, Cp, is also a carrier for iron. Dr Mondour and coauthors made a argument that the cardiac problems seen in the goats could have resulted from iron deficient anemia. [7] Creatine kinase is found in heart, skeletal muscle, and brain; finding it in the blood is a sign of damage.
lox, lysyl oxidase
Lysyl oxidase is a copper cofactor enzyme that cross-links collagen fibrils. DiNicolantonio and coauthors presented a compelling argument that this cross-linking contributes to the mechanical properties of the heart. [3] This group also thinks that advanced glycation endproducts are a problem in Cu deficiency. [3] The Fukai group discussed lox from the standpoint of vascular wound and the consequences of lacking the caperone Atox1 and the transporter ATP7A. [4] Liu and Miao also focused on collagen cross linking and mechanical properties of the heart. [5]
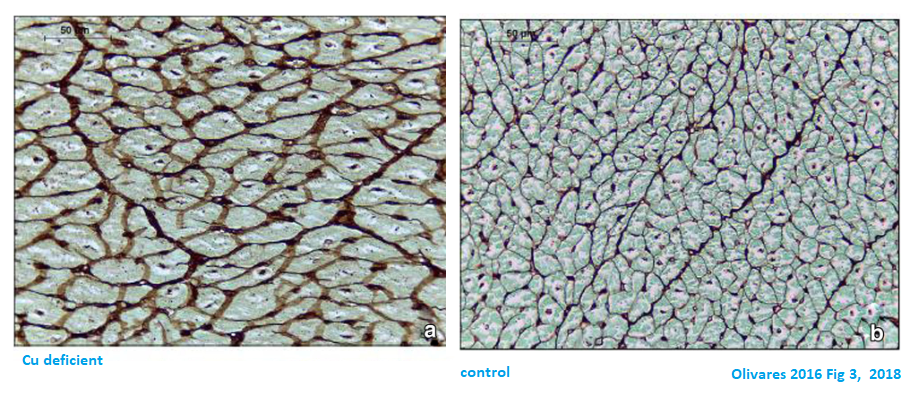
Fig. 2 Olivaras Area occupied with connective tissue. IS, interventricular septum;LV, left ventricle; RV, right ventricle; WM, whole myocardium. *Statistically different (P < 0.05) with respect to control Images have been added to show the chemistry of collagen cross linking and formation of advanced glycation end products.
The GMS stain reacts with carbohydrates. If lysyl oxidase is under active, the aldehyde form of glucose could react with the side chains of lysine that have not undergone the oxidation to the allyl lysine form (above).
Fig. 3 Histopathological image of left ventricle myocardium stained withGMS, × 400. Deficient animals showed a severe thickening of myocytes basement membranes (a) with respect to control group (b)
cytochrome C oxidase..ATP to power the heart beat
Or not. Copper deficiency may be linked decreased Cox activity and ultimately cardiac hypertrophy. [3,5] Cardiac Cox was not significantly different between the adequate and deficient bovines. [6]
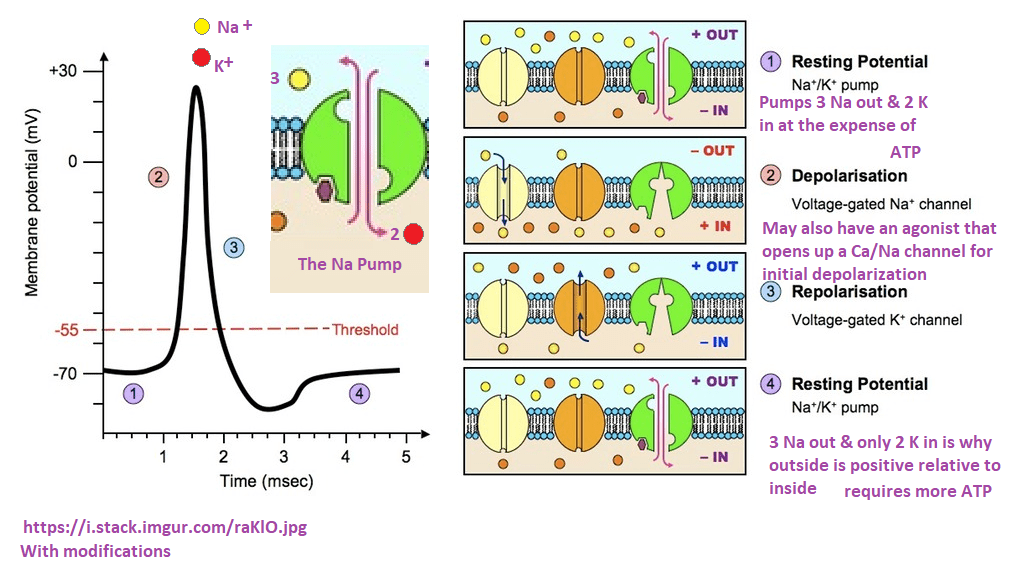
ATP and the action potential
Cytochrome C oxidase is a component of the mitochondria that makes ATP. ATP is an absolute requirement for the action potential That signals a post synaptic neuron to
Steps of the actin potential that apply to post synaptic neurons and to muscle.
Action potentials, in neurons and muscles require the ATP fueled Na Pump to return to the resting membrane potential. Muscle contraction requires to other ATP intensive processes. The action potential in muscle travels to the DHP Ca2+ channel that signals the Ryanodine (& caffeine) receptor to release even more Ca2+ from the sarcoplasmic reticulum. Ca2+ binds to TnC of the troponin complex that moves tropomyosin aside so that myosin heads may move about on actin. This of course requires ATP! Getting Ca2+ back into the SR requires ATP!
The makers of CopperOne have a tendency to want to make everything about ATP and the mitochondria. Let us continue this journey that leads to Cu/Zn SOD and lysyl oxidase.
Mandour et al ECG and echo data
This is an extremely nice study by a group of physiologists.
ECG data
Electrocardiogram (ECG) is a recording of the heart’s electrical activity during the cardiac cycle. The ECG is a graph of electrical potential difference detected by electrodes placed on strategic places on the skin … as a function of time.
Fig. 1 Mandour (2021) Illustrative electrocardiography obtained from the base-apex lead in Shiba goats. Normal sinus rhythm of goats showing rS (a) and qRs (b)patterns. Paper speed 50 ms;voltage 20 mv
Only specific intervals of the cardiac cycle were prolonged in the Cu deficient goats.
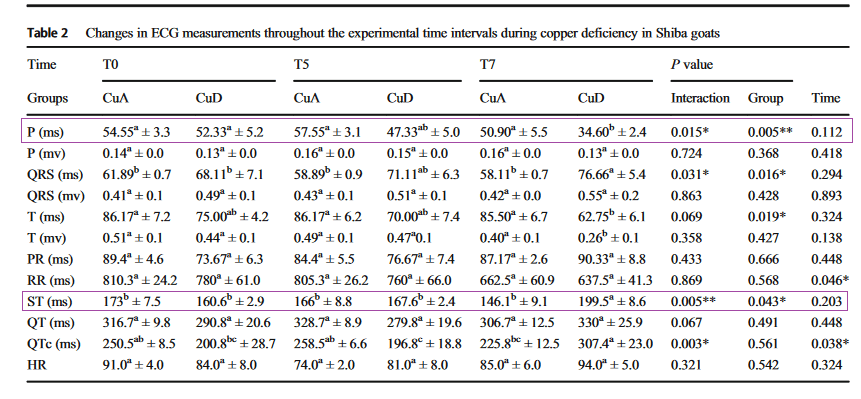
Mandour 2013 “Note: Values are expressed as mean ± SEM (n = 4). ECG obtained from base apex lead at three interval times presented as two-way ANOVA. Thelowercase letters are fitted for comparing means between groups. LSD <0.05. * P < 0.05 fitted to compare the significance of group, time, and interaction ms millisecond, mv milli volt, QTc corrected QT, HR heart rate”
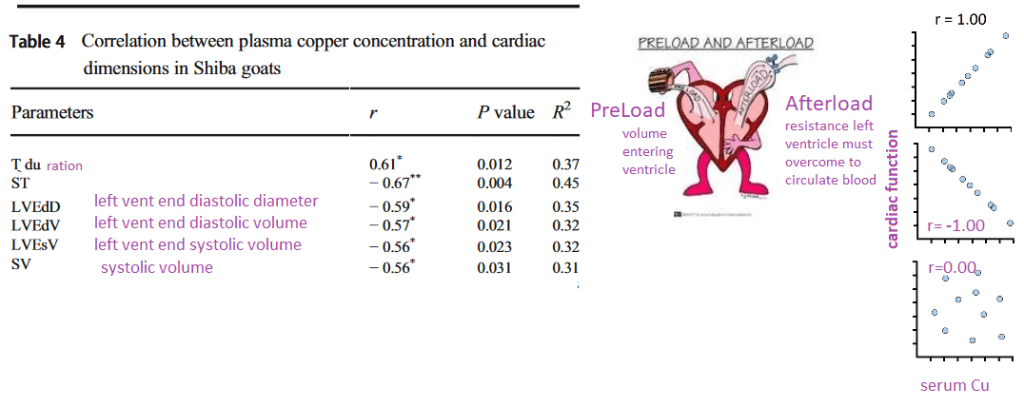
In the ECG data the P wave duration and the time between the QRS and T wave were the most influence by copper. Note that there was no change in heart rate as a result of copper deficiency. Changes in the ST segment are usually associated with ischemia. Indeed, a significant negative correlation was observed for the ST interval as a function of serum copper, see table 4 edited for only significant values. Graphs on the right hand side illustrate hypothetical correlations. The more copper, the longer the T segment duration.
Echo cardio data
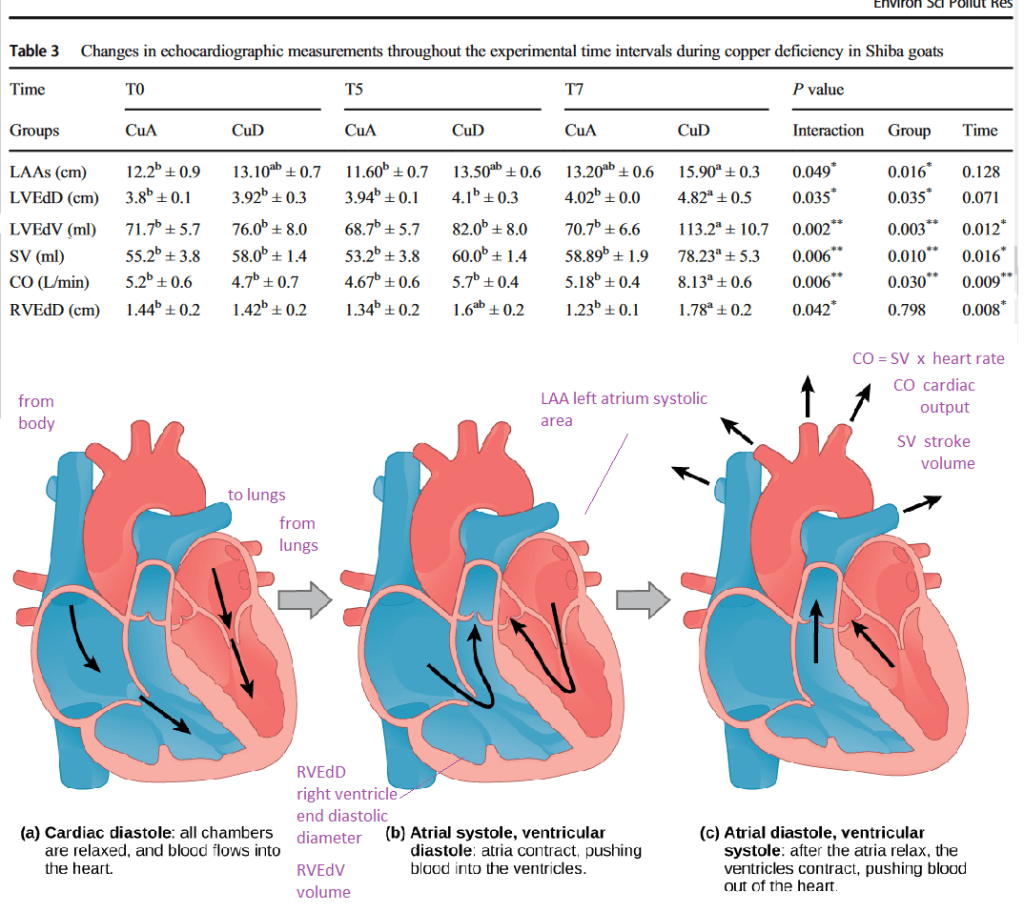
Table 3 from Mandour 2021 has been edited to show only the significant results. Some images of the cardiac cycle have been added for the non cardiologists. The cardiac output and stroke volumes have increased, the end volumes and diameters have also increased. It’s as if blood is moving through
Correlating heat data with serum copper content…
A highly edited version of Table 4 from Mandour 2021. Cartoons explaining preload and after load and correlation coefficient have been added for clarity.
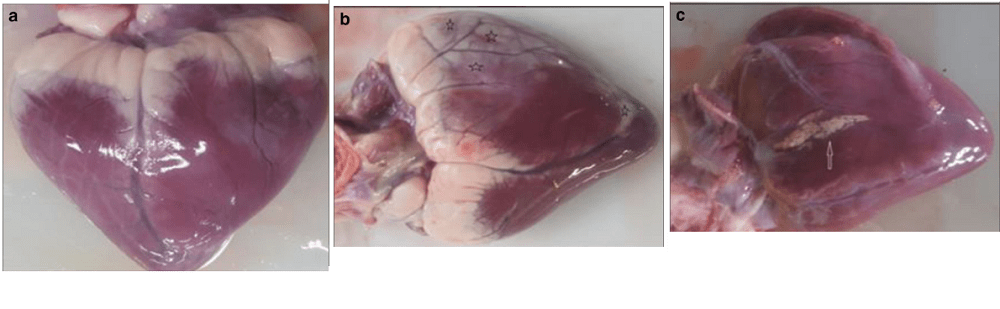
Dr Mandour and colleagues attributed the prolongation of the ECG parameters in the Cu deficient group at five and seven months to ventricular enlargement via hypertrophy or dilation. [7] They proposed that the reduced ECG T-wave duration may be due to cardiac damage as based up by increases in systolic volume, cardiac output, left atrium area, and so on in Table 3. Increased preload and cardiac dilatation were cited as possible explanations. [7] The preload is the extent of which the sarcomers are stretched before the heart contracts. Mandour and coauthors favored cardiac remodeling in response to anemia as the explanation. [7] Anemia results in decreased systemic peripheral resistance and thus a decreased afterload. Interestingly. anemia may arise from decreased plasma and cardiac Fe2+ secondary to the decrease in Cu. [7] In spite of these alterations, the copper deficient goats did not develop severe cardiomyopathy or heart failure. these are some images of goat hearts in the Mandour 2021 study. [7]
Mandour 2021 Fig. 3 Necropsy examination of the heart at the end of the experimental CuD in goats. a Normal appearance of the heart from the CuA (control) group showing no gross lesion. b Goat’s heart from CuD group showed a widespread of paleness, grayish streaks of myocardial degeneration, and necrosis (black stars). c Focal necrotic lesion on the external surface of the heart (white arrow)
Conclusions…
We’ve known from early studies of Leslie Klevay that Cu deficiency is associated with heart disease. [1,2] What we have posted about copper in regards to Covid-19 is more or less consistent with what experts in the heart have written about Cu deficiency and heart disease. [3-5] Olivares and coauthors found increased extracellular matrix and decreased serum and hepatic Cu in Cu deficient bovines. [6] Much of the Olivares report focused on mitochondrial defects. [6] Mandour and coauthors conducted and extensive cardiology study on Cu deficient goats. A concluding suggestion that secondary iron deficiency anemia might be cause of decreased after load and accompanying cardiac changes. [7] We could just as easily argue that a decrease in Cu/Zn SOD could allow super oxide to react with the blood vessel relaxing small molecule nitric oxide. We could also argue that changes in lysyl oxidase cross linking of collagen in blood vessels is important. The cartoon of Hatori and coauthors says it all. CCO might get first dibs when Cu is deficient. Lysyl oxidase being further down in the Cu “lunch line” may create long term problems.
Thoughts which copper enzymes are important in copper deficiency after reading the literature. The ones that are most important for short term survival may get Cu+ first based on affinity [8] but they may all be important in long term heart health.
This is the CopperOne summary_cartoon. Thank you for reading.
References
Klevay LM. (1973) Hypercholesterolemia in rats produced by an increase in the ratio of zinc to copper ingested. Am J Clin Nutr. 1973 Oct;26(10):1060-8.
Klevay LM, Viestenz KE. Abnormal electrocardiograms in rats deficient in copper. Am J Physiol. 1981 Feb;240(2):H185-9. doi: 10.1152/ajpheart.1981.240.2.H185. PMID: 7468813.
DiNicolantonio JJ, Mangan D, O’Keefe JH. Copper deficiency may be a leading cause of ischaemic heart disease. Open Heart. 2018 Oct 8;5(2):e000784. PMC free article
Fukai, T., Ushio-Fukai, M., & Kaplan, J. H. (2018). Copper transporters and copper chaperones: roles in cardiovascular physiology and disease. American journal of physiology. Cell physiology, 315(2), C186–C201. PMC free article
Liu, Y., & Miao, J. (2022). An Emerging Role of Defective Copper Metabolism in Heart Disease. Nutrients, 14(3), 700. PMC free article
Olivares RWI, Postma GC, Schapira A, Iglesias DE, Valdez LB, Breininger E, Gazzaneo PD, Minatel L. (2019) Biochemical and Morphological Alterations in Hearts of Copper-Deficient Bovines. Biol Trace Elem Res. 2019 Jun;189(2):447-455. free article
Mandour AS, Elsayed RF, Ali AO, Mahmoud AE, Samir H, Dessouki AA, Matsuura K, Watanabe I, Sasaki K, Al-Rejaie S, Yoshida T, Shimada K, Tanaka R, Watanabe G. The utility of electrocardiography and echocardiography in copper deficiency-induced cardiac damage in goats. Environ Sci Pollut Res Int. 2021 Feb;28(7):7815-7827. free article
Hatori Y, Inouye S, Akagi R. Thiol-based copper handling by the copper chaperone Atox1. IUBMB Life. 2017 Apr;69(4):246-254. free article
Mitochondria may be found outside the cell in four ways:
as cell free mitochondrial DNA in the plasma
encased in platelets
in exosome membranes
totally free
The authors of this review discuss the use of mitochondria isolated from the cerebral spinal fluid from sub arachnoid hemorrhage patients. [1] The mitochondria membrane potential indicator dye JCI was used to assess the health of released mitochondria. The origin of the mitochondria was determined by use of surface specific antigens in the flow cytometry system. [1] Mitochondria, in vesicles or not, may be taken up by new host cells. The Miliotis review discussed use of cell free mitochondria as a therapy. [1]
Exosomes and oxidative stress
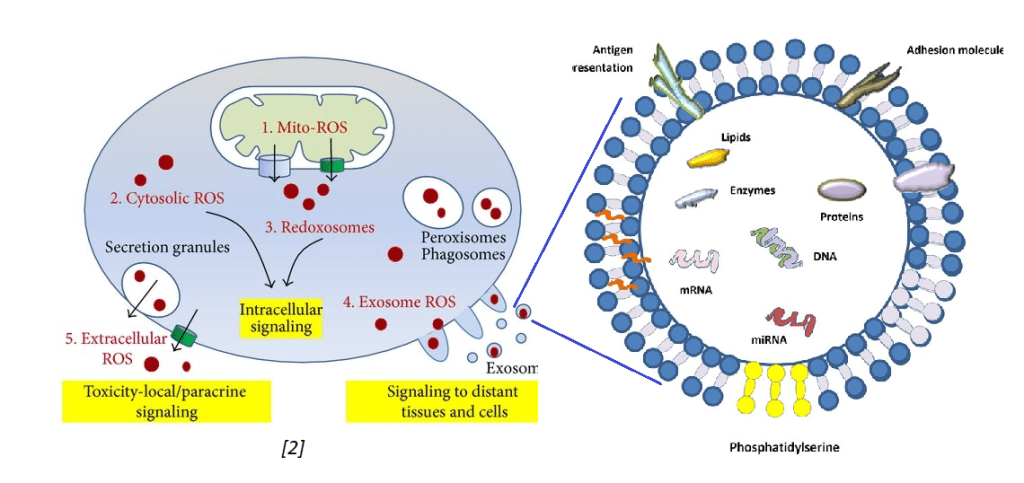
Tefani and coworkers (2016) published an excellent review on oxidative stress that touched briefly on mitochondria debris being exported into exosomes. [2] In their review of the literature, these authors stated that healthy cells do not secrete many exosomes. Stressed cells do. They also discussed exosomes containing reactive oxygen species such the super oxide anion.
The image on the left was extracted from the Tefani review. [2]
The other image just states that exosomes may contain messenger RNA (mRNA), micro RNA (miRNA), DNA, lipids, proteins, and presumably active protein enzymes. Exosomes contain protein antigens on their cell surface that my be used to identify their cell of origin. Exosomes are not only secreted by one cell type but may be absorbed by different cell types via antigen presentation and adhesion molecules. This is some background information for presentation of work done by the Goetzl Laboratory.
The Goetzl Lab general protocol
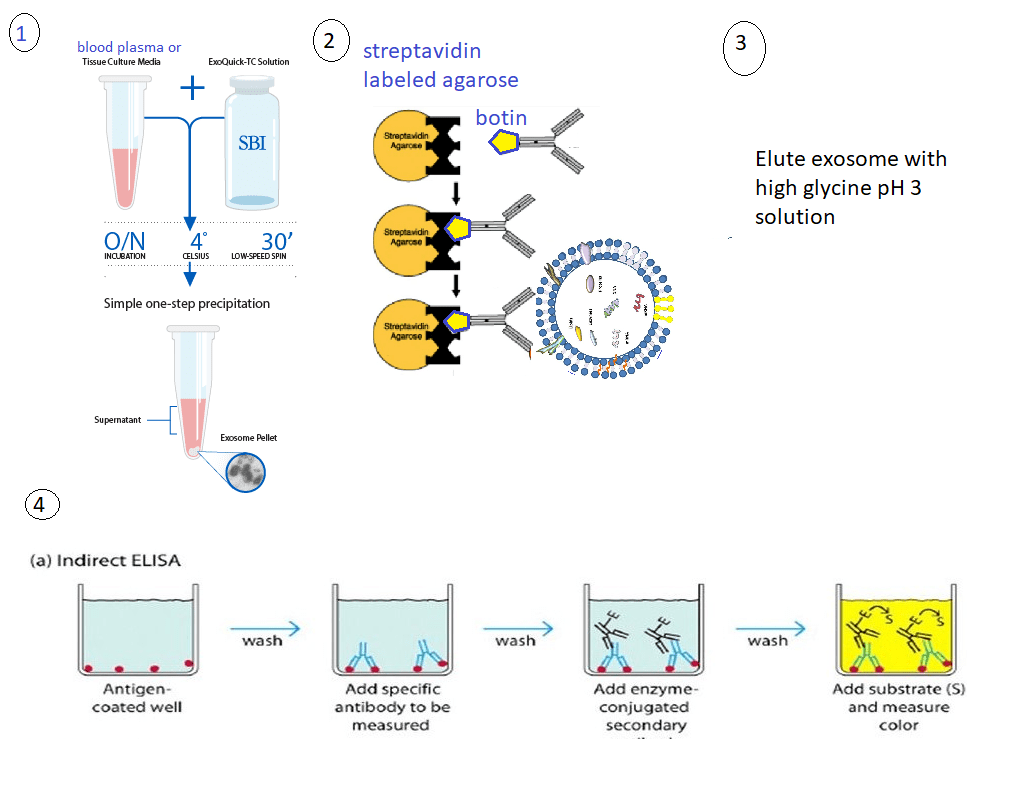
These protocol use only 0.25 mL of blood plasma that is then incubated with 0.1 mL of thromboplastin D for 30 min at room temperature for 30 minutes. A balance salt solution with protease and phosphatase inhibitors is added. The mixture is centrifuged at 3000xg at 4oC for 30 minutes. The supernatant was removed and exosomes precipitated with ExoQuik from System Biosciences. The total population of exosomal vesicles was resuspended in the balanced salt solution. Neuron or astrocyte specific antibodies were added. The primary antibodies may be conjugated with biotin. Biotin binds to streptavidin with extremely high affinity. The antibody labeled exosomes can be removed from the mix with streptavidin agarose beads. The eluted material was transferred to a tube containing 10% BSA and 1M Tris pH 8 to get the pH closer to physiological.
The general protocol 1. Exosomes are removed from blood plasma using a commercial kit. The pellet contains the exosomes. 2. Exosomes are reuspended in a solution. They can be sorted by tissue of origin by use of antibodies against surface proteins specific to that cell type. 3. The exsomes are eluted from the antibodies by use of a glycine solution. 4. Enzyme linked immuno sorbentassays
ELISAs were used for quantitation.
1. neuron or astrocyte derived exosomes in psychosis [3]
Goetzl and coworkers were tracking mitochondrial proteins in exosomes in major depression disorder patients at the baseline and after treatment with SSRI. This study is of interest to Mitosynergy because some of the customers take cuprous nicotinic acid for depression. This particular study was using SSRIs to treat some sort of self diagnosed depression. This particular study compared baseline values of responders and non-responders (NR) with the mitochondrial markers after treatment. (TR)
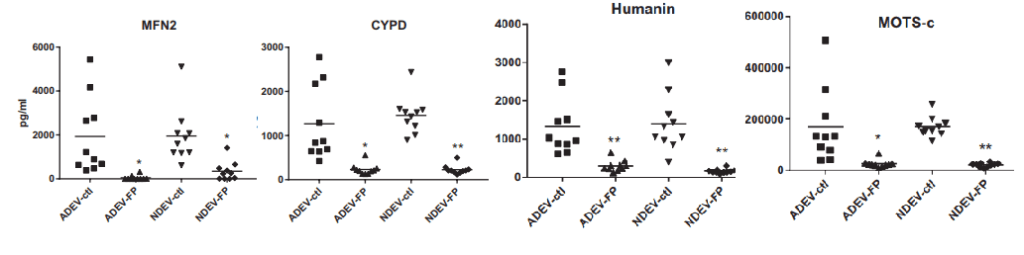
These are some highlights from Goetzl (2021) Figures 1. [3] Not shown are TFAM, MYO6, and LETM1
Mitofusin 2 (MFN2) Involved in the clearance of damaged mitochondria via selective autophagy (mitophagy) (PubMed:23620051). Is required for PRKN recruitment to dysfunctional mitochondria (PubMed:23620051).
Cyclophilin D (CYPD)has multiple functions in ghe mitochondria. Perhaps most notable is regulation of the mitochondrial transition permeability pore with its binding partner VDAC, the voltage dependent anion channel.
Humanin is a 24 amino acid mitochondrial genome coded peptide. It prevents the formation of Abeta 42 amyloid products. Human also protects neurons from diverse challenges, suppresses apoptosis, preserves synaptic proteins, reduces neuroinflammation and regulates aspects of glucose metabolism.
MOTS-c In response to metabolic stress, translocates to the nucleus where it binds to antioxidant response elements (ARE) present in the promoter regions of a number of genes and plays a role in regulating nuclear gene expression in an NFE2L2-dependent manner and increasing cellular resistance to metabolic stress (PubMed:29983246). Increases mitochondrial respiration and levels of CPT1A and cytokines IL1B, IL6, IL8, IL10 and TNF in senescent cells
The nicotinic acid two thirds of Cu(I)NA2
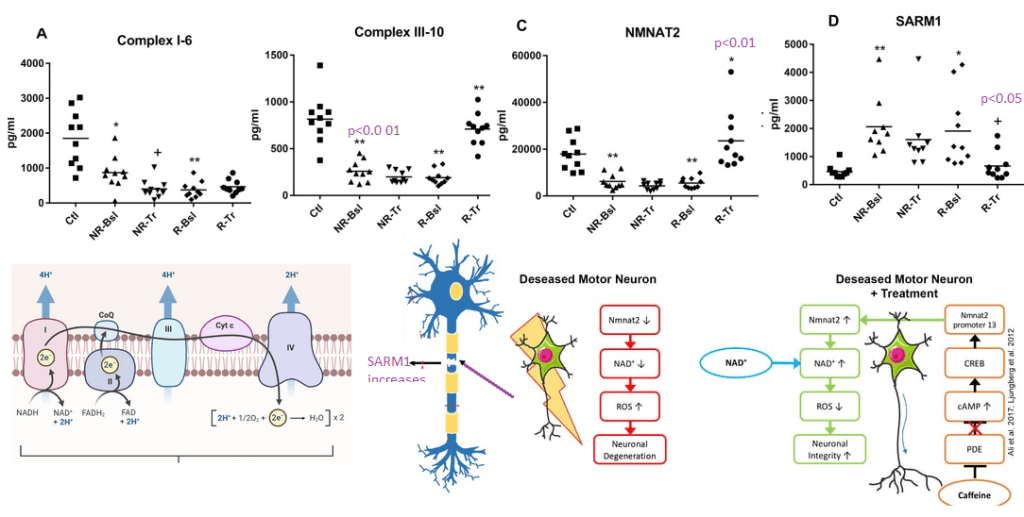
The Goetzl group may have chosen these proteins as specific electron transport chain proteins. They are of particular interest to mitosynergy because they involve the nicotinic acid derivative NADH.
Figure 2 from Goetzl (2021) [3] with some images from the Internet to illustrate the potential role of nicotinic acid as a precursor of NAD+.
NDUV1 6th unit of complex I ubiquinone + 5 H+(in) + NADH = ubiquinol + 4 H+(out) + NAD+
UQCR11 10th sub unit of complex III
NAD+ hydrolase SARM1 acts as a negative regulator of MYD88- and TRIF-dependent toll-like receptor signaling pathway by promoting Wallerian degeneration, an injury-induced form of programmed subcellular death which involves degeneration of an axon distal to the injury site.
2. In Alzheimer’s disease [4]
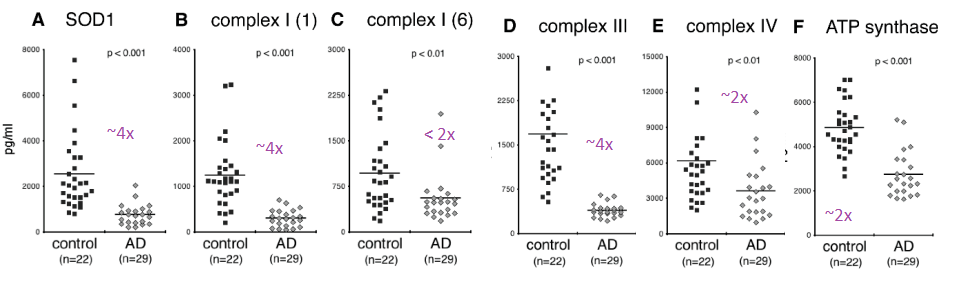
Complex IV was immunocaptured and assayed for its ability to reduce cytochrome C using a commercial kit. What is reported in this publication as ATP synthase activity is really Complex V operating in reverse as an ATPase.
From Yao figure 2 [4]
Figure 2 of the Yao (2021) is a bit perplexing. A n approximately 4x reduction in subunit 1 of complex I was seen in the Alzheimer’s group compared to the controls. There was an only 2x fold reduction of subunit 6 of complex I in the Alzheimer’s groups. Complex IV and V were observed to be about 50% less in the Alzheimer’s group compared to the control group. One possibility is that sub unit 1 of complex I is selectively damaged in AD. The authors did not mention if they detected the mitochondrial super oxide dismutase Mn SOD2.
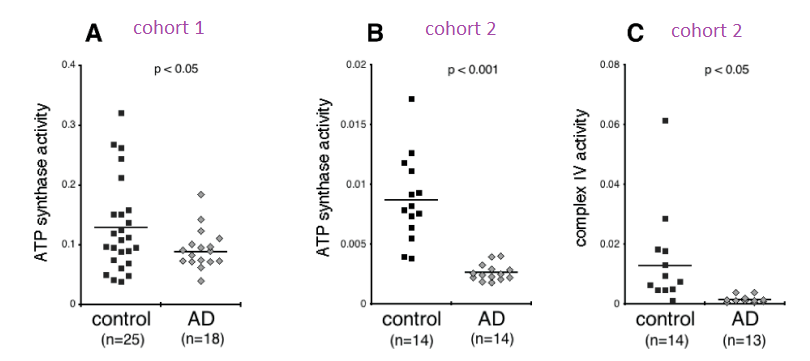
Two different cohorts were used for the ATPase assay. The activity in the Alzheimer’s patients was less than half than the controls in the first cohort and 3-4x less In the second cohort. Very little cytochrome C reductase activity was detected in the exosomes of Alzheimers’ patients in the second cohort. The complex IV activity was undetectable in the Alzheimer’s patients even though protein was detected. The Cu/Zn SOD1 activity was not assayed for in this study. Both Cu/Zn SOD1 and complex IV use copper as a cofactor. It would be interesting to measure the copper content of these exosomes. Being from Alzheimer’s patients, we’d need to know if copper is complexed to proper enzymes or to amyloids.
3. In neuropsychiatric PASC [5]
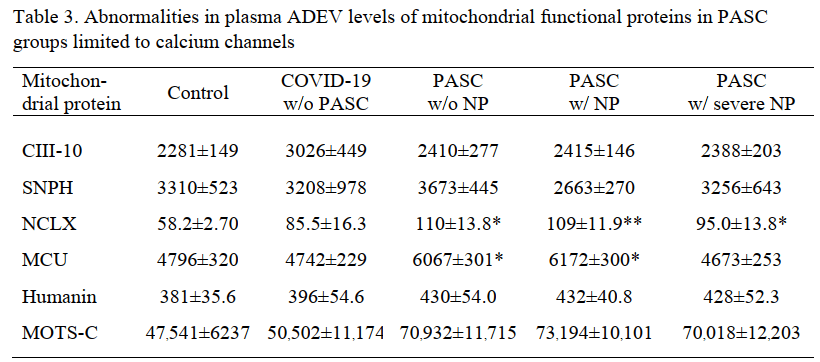
The Goetzl group published a study comparing patients with PASC with and without neuro psychiatric (NP) symptoms. Protein levels, but not enzyme activities, were published in this study. The truly incredible finding in this study was the presence of the Covid S1 spike protein receptor binding domain (RBD) and the nucleocapsid proteins.
N = nucleocapsid protein, NP = neuropsychiatric manifestations, RBD = receptor-binding domain, w/=with, w/o= without. Each value is the mean pg/ml±SEM. Statistical significance of differences between each value and the control value were determined by an unpaired Student’s t test: †, p<0.05; **, p<0.001.
The S1 spike protein immuno reactivity was about 3x greater in the asymptomatic former Covid patients compared to those that never had Covid. Some background is to be expected in any immuno detection assay. With the prospect of PASC having an autoimmune aspect needs to be considered in this system. The S1 spike protein was increased in even asymptomatic former Covid patients in both the neuronal and the astrocyte derived exosomes. The same spike protein was almost doubled in PASC patients with or without neuropsychiatric (NP) symptoms.
The nucleocapsid protein (N) immunoreactivity was significantly greater in NDEV in asymptomatic former Covid patients compared to those that never had Covid, the difference was less than 2x. In the astrocyte derived ADEV , nucleocapsid immunoreactivity became a predictor of neuropsychiatric symptoms.
The significant changes in host mitochondrial proteins were seen in the astrocyte derived exosomes.
The mitochondrial Na+/Ca2+ exchanger was the only protein that was increased even 2x.
Cool implications for Mitosynergy
The Goetzyl assay has a certain amount of simplistic beauty. Two unanswered questions are how these exosomes get past the blood brain barrier and whether FDA would accept this assay as a marker of efficacy. The latter may not be that important.
The MDD study that piggy backed on a clinical trial of effective and non effective SSRI was most interesting in that many of the enzymes analyzed had something to do with NAD+ pathways. Is some sort of Wallerian degeneration or other neurotoxicity associated with the etiology of major depression disease? Note: Mitosynergy and Charlie Barker’s patented improvement on cuprous nicotinic acid originated from his trip to Egypt for a treatment for his nephew’s spinal cord injury!
The Alzheimer’s Disease was truly incredible in that it examined the activity of complex IV and complex V going in reverse ATPase mode in exosomes. We’d like to see SOD1 activity measured. To the best of my knowledge, Alzheimer’s Disease is not an interest of Mitosynergy. Similar assays in spinal cord injury patients might be.
Mitosynergy is naturally interested in all aspect of Long Covid, now known as PASC. Astrosytes seem to be more effected. Is this due to their role as phagocytic role? Is seeing nucleo capsid protein in astrocyte exosomes a sign that they ore infected and/or that they are cleaning up debris from other infected cells? What markers to we want to see in healthy astrocytes that are doing their job versus reactive astrocytes?
References
Picca, A., Guerra, F., Calvani, R., Coelho-Junior, H. J., Bossola, M., Landi, F., Bernabei, R., Bucci, C., & Marzetti, E. (2020). Generation and Release of Mitochondrial-Derived Vesicles in Health, Aging and Disease. Journal of clinical medicine, 9(5), 1440. free paper PMC free article
Tafani, M., Sansone, L., Limana, F., Arcangeli, T., De Santis, E., Polese, M., Fini, M., & Russo, M. A. (2016). The Interplay of Reactive Oxygen Species, Hypoxia, Inflammation, and Sirtuins in Cancer Initiation and Progression. Oxidative medicine and cellular longevity, 2016, 3907147. PMC free article
Goetzl EJ, Wolkowitz OM, Srihari VH, Reus VI, Goetzl L, Kapogiannis D, Heninger GR, Mellon SH. Abnormal levels of mitochondrial proteins in plasma neuronal extracellular vesicles in major depressive disorder. Mol Psychiatry. 2021 Dec;26(12):7355-7362. PMC free article
Yao PJ, Eren E, Goetzl EJ, Kapogiannis D. (2021) Mitochondrial Electron Transport Chain Protein Abnormalities Detected in Plasma Extracellular Vesicles in Alzheimer’s Disease. Biomedicines. 2021 Oct 31;9(11):1587. doi: 10.3390/biomedicines9111587. PMC free article
Peluso MJ, Deeks SG, Mustapic M, Kapogiannis D, Henrich TJ, Lu S, Goldberg SA, Hoh R, Chen J, Martinez EO, Kelly JD, Martin JN, Goetzl EJ. (2022) SARS-CoV-2 and mitochondrial proteins in neural-derived exosomes of COVID-19. Ann Neurol. 2022 Mar 13 PMC free article
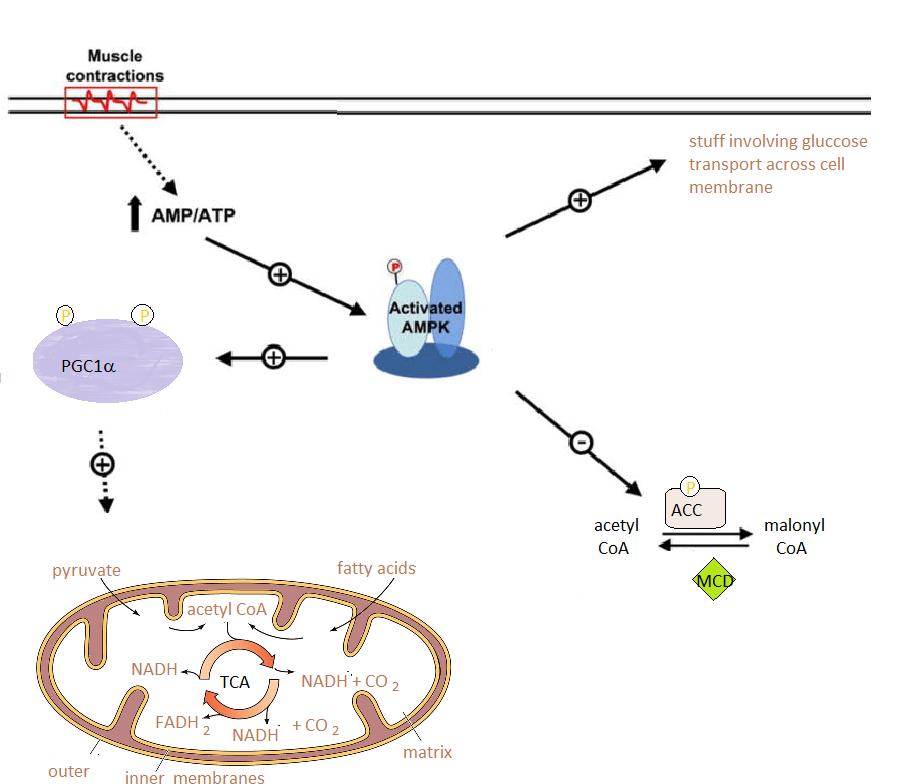
Uguccioni G, Hood DA. The importance of PGC-1α in contractile activity-induced mitochondrial adaptations. Am J Physiol Endocrinol Metab. 2011 PMC free article
Introduction
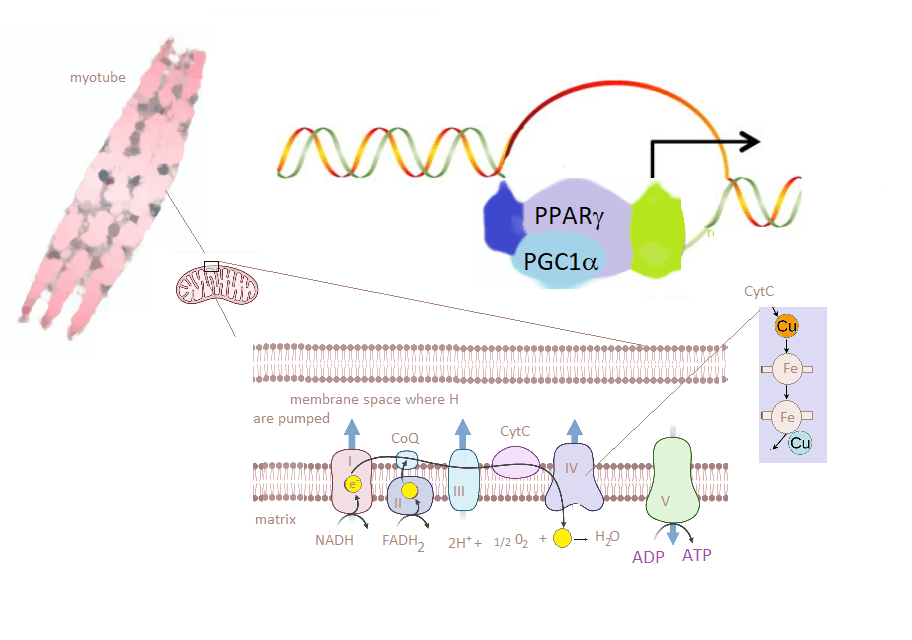
skeletal muscle has the ability to adapt to changes in metabolic demands by production of more proteins. Chronic contractile activity (CCA) is one of those metabolic demands. CCA results in production of more mitochondria. Only about 1% of the proteins in the mitochondria electron transport chain are coded for by mitochondrial DNA. The muscle must derive these transcripts from the chromosomal DNA in the nucleus. Prior to the featured study, peroxisome proliferator-activated receptor (PPAR)γ and its coactivator-1α (PGC-1α) were deemed critical to mitochondrial function, respiration, and biogenesis in skeletal muscle. Changes in PGC-1α mRNA correlated with changes in mitochondrial content as measured by cytochrome c oxidase (COX) activity. The scienific community had data from PGC-1α-knockout mice that were able to adapt to an exercise program and some contrasting data from animals with a muscle-specific deletion of PGC-1α. These authors used a contractile myotubule cell culture approach. To assess the role of PGC-1α they used silencing RNA to prevent the PGC-1α transcript from being translated into proteins.
The purpose of the electron transport chain is to transport electrons (yellow circles) from NADH and FADH2 to O2. H2O is the byproduct. H+ are pumped into the membrane space. Energy from this gradient is used to generate ATP. Complex IV contains 13 subunits. Cox IV contains two coppers and irons (Fe).
Some how or another CCA increases the protein levels of PGC-1α. We can hypothesize that this is somehow linked to ATP and its depletion by too much activity. PPAR)γ, PGC-1α and some other proteins increase the transcription of genes that code for mitochondrial proteins.
Methods
C2C12 murine skeletal muscle cells were proliferated in a nutrient rich medium containing some antibiotics and fetal bovine serum. When they became a bit crowded the fetal bovine serum was switched to adult horse serum. The result was myotubes that could contract in their comfy cell culture dishes.
Two platinum wire electrodes 2 cm apart were inserted into the culture dish. Myotubes were subjected to electrical stimulation at a frequency of 5 Hz and an intensity of 9 V chronically for 3 h/day over 4 successive days shortly after they differentiated. Myotubes were allowed to rest for 21 h after each bout of contractile activity. The changed the medium 1 hr before exercise. This Chronic Contractile Activity went on for four days, proteins and messenger RNA (mRNA) were extracted.
Results
The cell culture model was validated by showing that CCA increased COX activity as well as O2 consumption. The silencing RNA was successful in decreasing PGC-1α mRNA levels to about 30% of the control.These results gave Uguccioni and Hood confidence in their model
CCA increased protein levels of mitochondrial transcription factor Tfam and cytochrome C. PGC-1α silencing slightly decreased protein levels in resting but not CCA myotubules. Chronic contracting seemed to overcome this deficiency. This was not the case for COX IV. Because the silencing of was not complete, Uguccioni and Hood were able to show a nice, linear correlation between PGC-1α mRNA and COX activity.
Chronic Contraction causes depletion of ATP and an increase it AMP. This activates autophosphorylation of AMPKinase. In addition to phosphorylating itself, PKA was shown to phosphorylate ACC which inhibits ACC and shifts the balance to acetyl CoA, which can be used by the mitochondria in the TCA cycle, which generates NADH and FADH to make ATP.
AMP protein kinase is an enzyme that communicates decreases in ATP (adenosine triphosphate) and subsequent increases in adenosine monophosphate (AMP). AMPK accomplishes this task by attaching a phosphate to proteins starting with itself. Other targets include acetyl-CoA carboxylase 1 (ACC1) factors related to glucose trasnportacross the cell membrane. According to UniProt, PGC-1α has two AMPK phosphorylation site: threonine 178 and serine 539. Knocking down PGC-1α with silencing RNA increased some of these phosphorylations. We can hypothesize the myotubules not expanding mitochondria like nature intended them to.
Conclusion
This is how weight lifting increases mitochondria. There seems to be a huge link to COX IV and PGC-1α. The body builder may want to consider a copper supplement and then an iron supplement as these are cofactors in COX IV. Copper comes before iron because copper is required to absorb iron. See the ceruloplasmin post. CopperOne is just a more natural copper supplement because it is in the +1 oxidation state just like the Cox17 chaperone that loads cytochrome C oxidase of complex IV with Cu+1.
The reports keep coming in. This update is all about muscle autoantibodies. A group out of the UK compared auto-antibodies from 84 Covid-19 patients with 32 individuals who had been in the intensive care unit for other reasons. The Covid-19 group was subdivided into 24 who had mild symptoms that did not require hospitalization, 25 with severe Covid-19 whose blood was drawn while in the intensive care, and 35 who had severe Covid-19 whose blood was drawn 3-6 months into recovery. [1] Groups 1-4 were scored via the WHO ordinal Covid-19 severity scale.
1
no
Covid
2
acute
3
severe
6 mo
4
mild
6 mo
pos
tot
%
pos
tot
%
pos
tot
%
pos
tot
%
parietal cell
2
27
7.4
0
25
0
11
36
30.6â€
4
24
16.7
smooth
2
27
7.4
0
25
0
11
36
30.6â€
4
24
16.7
skeletal
1
25
4
4
24
16.7
7
36
19.4**
0
24
0
cardiac
2
21
9.5
1
14
7.1
10
36
27.8***
0
24
0
Table 1 2 ref [1]Only showing tissues for which there are images. All autoantibodies are IgG [1]. ** p = 0.02 (group 2 versus group 3) *** p = 0.005 (group 3 versus group 4). †p = 0.006 (χ2 comparing all groups).
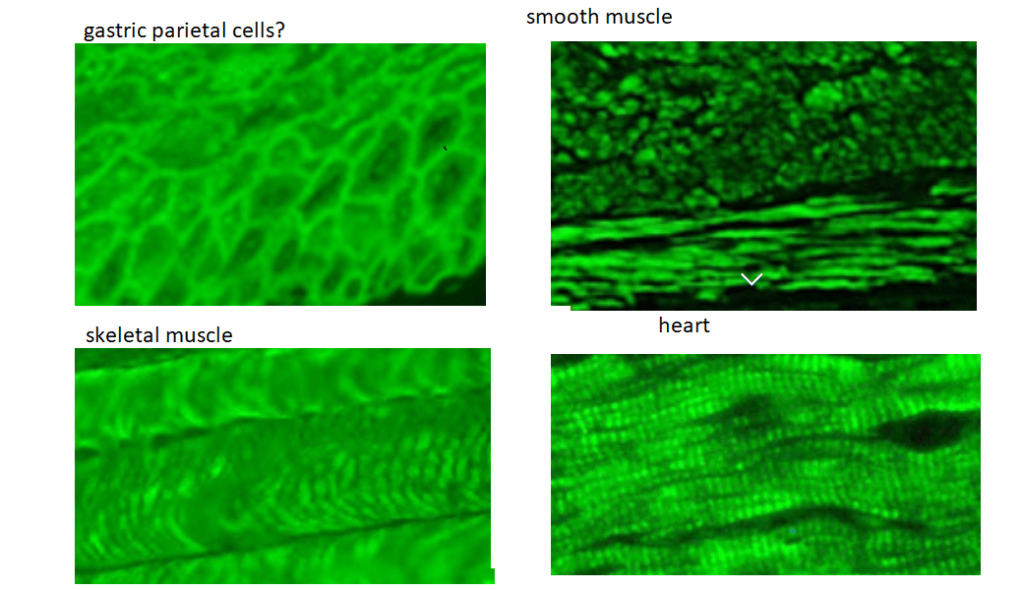
The bottom line is that these antibodies are staining areas that also contain the cytoskeleton protein β-actin.
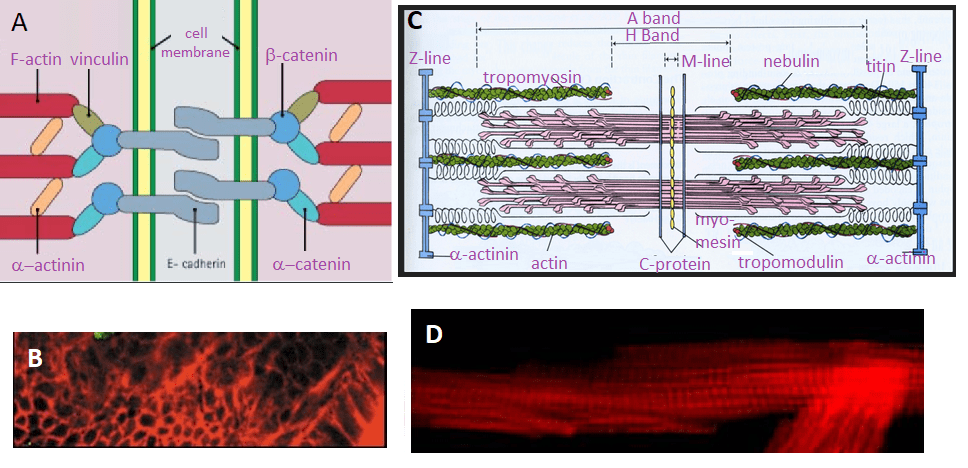
Figure 1 Some close ups of Figure 2 ref [1]
Rhodamine phalloidin is a dye that binds to this protein called actin. An internet search was performed to find images of gastric parietal cells minus ulcer causing bacteria, heart,
Figure 2 Making sense of Figure 2 of reference [1]. A. Cell adhesion junctions adapted from StudyBlue. B. Actin stainiing of paretal cells. C. The sarcomer from Study Blue. Is valid for both cardiac and skeletal muscle. D. Actom staomomg of cardiac muscle. The red fluorescence corresponds to the A-band.
There is a light area of disagreement with X-axis title in Figure 2 that is a bar graph that lists the percentage of patients in the four groups as a function of the independent variable of 0, 1, 2, and 3 auto antibodies. The heart and parietal cell auto antibody staining looks very much like actin staining with rhodamine phalloidin. Actin and α-actinin are proteins common to parietal cells and the three types of muscle. An autoantigen against α-actinin released from airway or GI tract epithelial cells may cross react with α-actinin isoforms found in smooth, skeletal and cardiac muscle. The Wikipedia actin page list the six isoforms of mammalian actin. This particular Wikipedia page has grown quite extensively in its coverage of the many binding partners of actin in multiple tissue types. The “tissue specific” auto antibodies that very much align where we expect to see actin, could be recognizing actin or anything that binds to actin.
A group out of the United Kingdom took a different approach:
They purchased recominant human IgG1 monoclonal antibodies made against Covid-19 spike protein S1 and S2 domains and SARS-CoV-2 nucleoprotein. [2]
They purchased the following purified proteins: cardiolipin, actin, myelin basic protein (MBP), tropomyosin, ganglioside GM1, insulin, liver microsomes, transglutaminases (tTGs), enolase, beta-amyloid protein, tau protein, somatotropin, human serum albumin (HSA), and dipeptidylpeptidase.
The ability of human and rabbit Covid-19 antibodies to react with their assortment of purified proteins was tested. They used optical density (OD) using an ELISA assay.
Portions of the sequences of Covid-19 proteins were aligned with cytoplasmic actin
Antigens
Spike protein OD
% reactivity
Nucleo protein OD
% reactivity
Envelope protein OD
% reactivity
Membrane protein OD
% reactivity
SARS-CoV-2
3.4
100 ++++
3.76
100 ++++
3.68
100 ++++
3.78
100 ++++
Actin
0.74
17.6 +
1.1
27.1 ++
0.78
18.0 +
0.95
22.2 +
NFP
1.98
56 ++++
0.42
8.5 +
0.27
3.7 –
2
51.1 +++
Alpha-myosin
0.72
17.0 +
0.89
21.3 +
0.36
6.2 +
0.94
21.2 +
Tropomyosin
0.21
1.2 –
0.25
3.8 –
0.25
3.1 –
0.58
12.1 +
Int epi cells
0.49
9.9 +
0.46
9.6 +
2.13
56.0 ++++
0.95
22.2 +
Table 2 From Table 1 reference [2] OD, optical density; NFP, ; Int epi cells, intestinal epithelial cells
SARS-CoV-2 antigen
SARS-CoV-2 sequence
Mapped start to end
Actin sequence
ID (%)
Chain A, Spike protein
GKIQDSLSST
16–25
GSILASLS-T*
60
Chain A, Spike protein
STEKSNII
85–92
STMKIKII*
63
Chain A, Spike protein
IGAGICAS
697–704
IGGSILAS*
63
Chain A, Spike protein
PS–GRLVPR
1,210–1,217
PSIVGR–P
60
Chain A, Nucleoprotein
SSSTKKS
15–21
SSSLEKS
71
Chain A, Nucleoprotein
TEGALNTPK
90–98
TEAPLN-PK
67
Chain A, Spike protein
SVLYNSASFSTF
33–44
SIL—ASLSTF**
58
Chain B, Spike protein
SVLYNSASFSTF
48–59
SIL—ASLSTF**
58
Chain C, Spike protein
SVLYNSASFSTF
48–59
SIL—ASLSTF**
58
Chain E, Spike protein
SVLYNSASFSTF
37–48
SIL—ASLSTF**
58
Chain E, Spike receptor binding domain
SVLYNSASFSTF
48–59
SIL—ASLSTF**
58
FTable 3i From reference [2] regions of Covid-19/SAR-Cov2 that share homology with human β actin.
The human cytoplasmic β-actin as protein blasted against the human database. β-actin shares 94-99% sequence homology to the other five isoforms of mammalian actin.
Figure 3 Blastp results from www.ncbi.nlm.nh.gov/protein
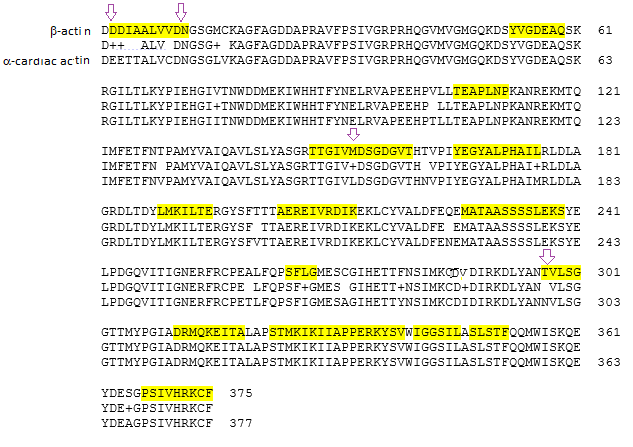
Since we have been examining cardiac tissue in Figure 1 and 2, Figure 3 shows the alignment between and cardiac actin. The top line is the sequence of β-actin, the third cardiac actin, and the middle the sequence homology. A “+” indicates substitution with a similar amino acid . Regions that share homology with Covid protein are highlighted. Note that these overlapping regions also share homology with cardiac actin. Table 5 from reference [2] contains some homology between non spike proteins and β-actin. These include some non structural proteins and helicases.
Figure 4 Alignment of β-actin and cardiac actin with sequences homologous to all the Covid-19 proteins discussed in reference [2]
Coivd-19 patient sera certainly seem to have antibodies that bind to actin in a variety of tissue sections. [1] This report stopped short of showing that these polyclonal antibodies actually recognized actin. [1] Another report demonstrated binding of human recombinant monoclonal antibodies can recognize purified actin. [2] This report offered some nice speculations as to molecular mimicry with the spike protein and other Covid proteins. The implication of the latter report are interesting in that they suggest the potential for developing a Long Covid auto immune disorder from the vaccine. Finally, autoantibodies against an extremely abunant protein like actin imply a major immune response to even a slight injury that releases actin into the circulation. The high degree of homology between actin isoforms of actin only more problematic.
References
Richter AG, Shields AM, Karim A, Birch D, Faustini SE, Steadman L, Ward K, Plant T, Reynolds G, Veenith T, Cunningham AF, Drayson MT, Wraith DC. Establishing the prevalence of common tissue-specific autoantibodies following severe acute respiratory syndrome coronavirus 2 infection. Clin Exp Immunol. 2021 Jun 3. free article
Vojdani, A., Vojdani, E., & Kharrazian, D. (2021). Reaction of Human Monoclonal Antibodies to SARS-CoV-2 Proteins With Tissue Antigens: Implications for Autoimmune Diseases. Frontiers in immunology, 11, 617089. PMC free article
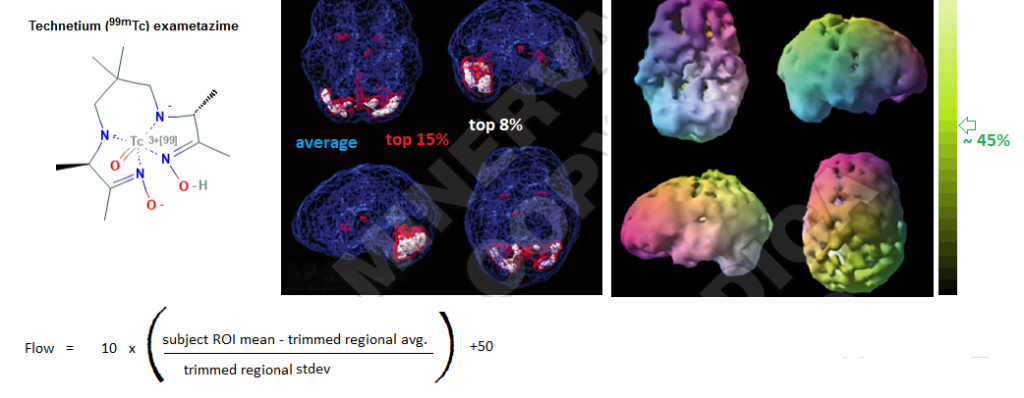
This post covers work of Daniel Amen. .. ir just a very small bit of a large amount. Dr Amens has become a celebrity over promoting SPECT imaging, “blood Flow” through various regions of the brain, and of course brain directed nutrients to restore “blood flow” to normal. Purists may associate “flow” with a unit volume per unit time such as mL per minute. Mayo Clinic breaks down single-photon emission computerized tomography (SPECT) imaging in simple steps: (1) inject patient with γ radiation emitting compound. (2) The patient allows the compound to partition from blood to tissues of the body for 20 minutes or more. (3) The image is acquired. (4) The patient is asked to drink plenty of fluids to encourage the compound to partition back into the blood where it can be eliminated in the urine.
What am I looking at?
Technetium (99mTc) exametazime is very simply a radioactive agent that emits a photon of the gamma radiation wavelength. It is used to measure blood distribution in tissue. It should not be confused with Fluorodeoxyglucose (18F) used in positron emission tomography PET. The latter measures uptake of glucose assumed to be related to the metabolic activity of a tissue. The active rendering of blood flow is petty straight forward. One just needs to be constantly aware of the color code.
Technetium tc 99m exametazime is the gamma photo emitting agent to measure blood flow. The blue and white o,age represents active flow from, reference [1] Figure 2. The rainbow images are from reference [1] figure 4. The equation was used in the reference [2] study
The surface rendering is difficult for many to conceptualize. The colors themselves seem to have little bearing on the flow. Pure green, cyan, orange, and red are all the same flow going down into the brain. Gray shades of the colors indicate <45% of the average perfusion. [1]
You are looking at different renderings to make statements
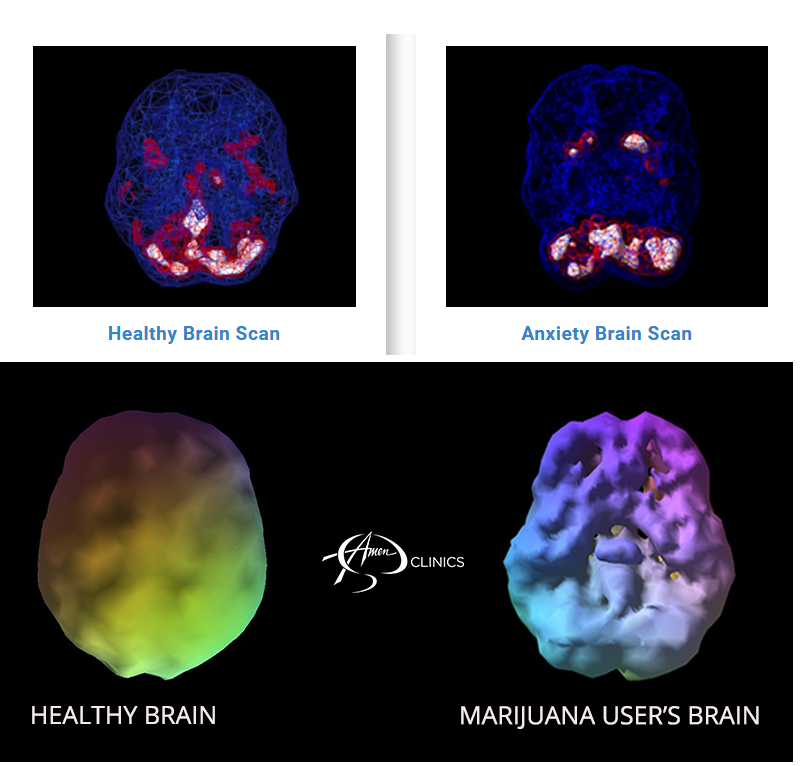
On an anxiety page the Amen group makes a point that there is high relative blood flow in the cerebellum of normal and in individuals with anxiety. Basal ganglia blood flow in the person with anxiety is high compared to the normal control. The activity rendering is an excellent way to locate the region of increased blood flow and gives the patient peace of mind that there is indeed something tangible out of order in their brain. It gives the psychiatrist some insight on possible medications. Interestingly, the sight on anxiety is linked to a sight on marijuana, a plant based medicine used to treat anxiety.
Both sets of images are from the amenclinics.com website.
The surface rendered healthy brain has some grayish dips indicating somewhat lower blood flow in regions below the surface. The cerebellum is bright and shiny smooth in this surface rendering of a healthy brain. The marijuana user’s brain is full of pot holes indicating substantial regions of decreased blood flow. We were not told how much THC was in the system of the patient at the time of the scan. Was this patient self medicating with mmj and just missed the mark by decreasing more than the intended brain activity? The “Swiss cheese” surface rendering of the mmj patient’s brain would make a more powerful statement than a nice, calm, mostly blue activity rendering. Finding surface abd activity plots of habitual coffee drinkers before and after the morning cup is a bit more difficult.
Excess body weight and brain blood flow
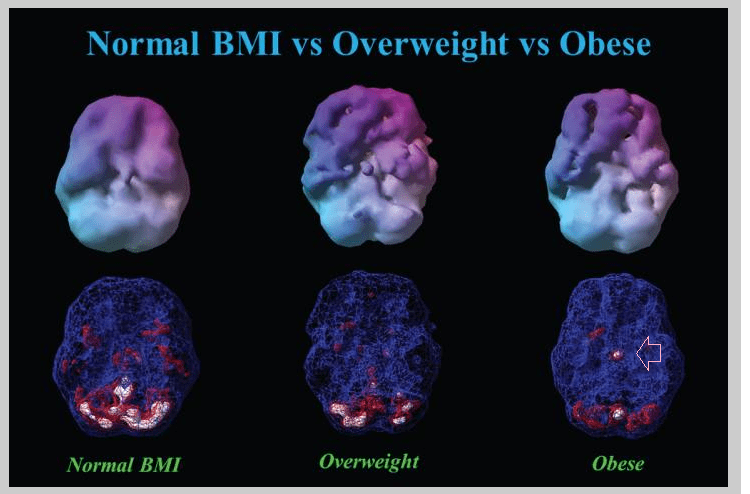
Blood flow was compared among the following group of patients: underweight (BMI < 18.5), normal weight (BMI 18.5–24.9), overweight (BMI 25–29.9), obese (BMI≥30), morbidly obese (BMI≥40). [2] All subjects received intravenous administration of an age- and weight-appropriate dose of technetium-99m hexamethylpropylene amine oxime (99mTc-HMPAO) for brain SPECT imaging. Each subject received a resting, or baseline, scan and a task. [2] What was not clear was if 99mTc-HMPAO partitioned into adipose tissue. If so, it would not be enough to simply assume that morbidly obese patients have more blood than their underweight counterparts.
From reference [2] Figure 6. All three subjects were 40 year old males. The arrow points to a region of hyper perfusion. This arrow did not appear in the original publication.
The authors reported a pattern across virtually all brain regions in which a decline in cerebral perfusion inversely correlated with BMI. Flow was best in the under weight and wose in the morbidly obese. [2] The authors reported no regions that showed elevated perfusion in relation to higher BMI. [2] To have a small region of hyper perfusion (arrow) suggests that decreased flow as BMI increases is not an artifact of the detector partitioning into adipose tissue.
The Brain Directed Nutrients (BDN) Clinical Trial
The Goal was to determine whether supplementation with BDNs improved cerebral blood flow CBF and neuropsychological function in healthy individuals. The participants were randomized to receive the BDN or a placebo for two months. [3] Neither the investigators nor the participants knew whether they were receiving the placebo or BDN. At the end of two months the groups crossed over. The placebo group got the BDN and the BDN group crossed over to receiving the placebo. [3] This study was conducted at the Amen Clinic in Newport Beach, CA. The participants included 30 locals, 15 of which were men and the other 15 women. Five participants failed to complete the study for reasons unrelated to the study. In a cross over design participants were given a baseline brain scan and then a placebo or brain directed nutrients for two months. At the end f this time they were given another brain scan and the same tests. Then the participants crossed over: the placebo group got the BDN and the BDN group got the placebo for two months. At the end of four months the participants were given a third brain scan and the same tests.
The treatments
fish oil, 2.8 g per day
multivitamins and minerals that include 1mg copper glycinate and 30 mg nicotinamide
A mixture of small molecule anti oxidants and hormone modulators that included huperzine A, Ginkgo biloba, and N-acetyl cysteine and sodium/copper chlorophyllin
some digestive enzymes, which are technically large molecules, were also included
In the placebo treatment rice flour to replace all BND components except the fish oil. A mixture of undisclosed vegetable oils was used to replace the fish oil.
Outcome measures, results
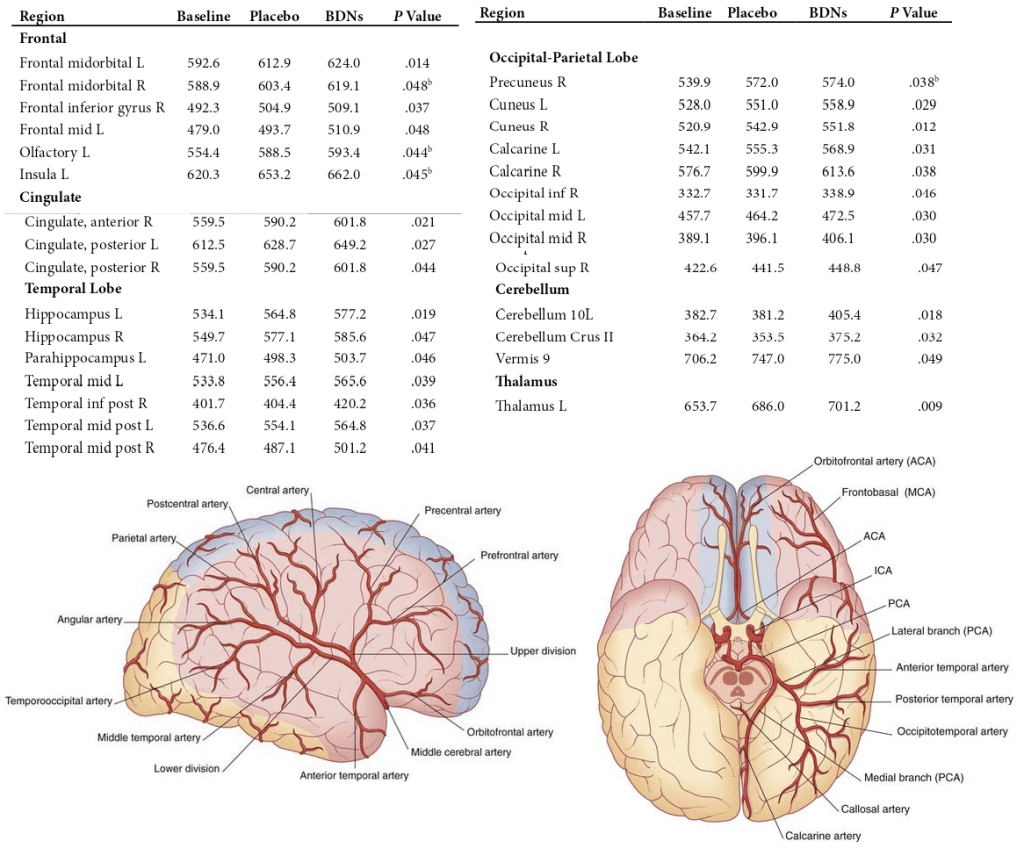
Let’s take a look at a table reporting significant changes in well defined regions of the brain. Some images of major blood vessels in the brain are included to make a point that changes in blood flow depend on smooth muscle in the major vessels as well as smaller arterioles and venules.
Table from reference [3] https://neupsykey.com/blood-supply-of-the-brain/
As one might expect, cognitive test scores improve the more times the test is taken.
aInteraction of treatment order and treatment condition for memory; means and 95% confidence intervals are shown. The response is linear when BDNs are given first compared to a quadratic response when BDNs are given second, regressing from baseline to treatment to placebo[3]
Significant improvements were observed for the BDNs
MicroCog—reasoning, P = .008
memory, P = .014
information processing accuracy, P = .027
WebNeuro—executive function, P = .002
information processing efficiency, P = .015
depressed mood, P = .017
emotional identification, P = .041
BSI—positive symptom total, P = .024
A reduction in the hostility score was seen. P = .018. Adjusting for the effect of order was required to reach significance. [3]
Conclusions… sort of
It is fairly easy to see why Dr Daniel Amen has achieved celebrity status with his mixture of psychiatry and SPECT imaging. He sells peace of mind of seeing proof that something no so good is going on in a person’s brain in a non insurance funded sort of way. Proper presentation of the data can encourage and/or guide healthy living. In true MD fashion, the BDN are “everything but the kitchen sink” to reduce oxidative stress that might be causing reduced blood flow, excitotoxicity, and so on. This latter was not a study to establish a mechanism. The trial did offer convincing evidence that the Amen group is on the right tack.
References
Amen D. Brain SPECT imaging in clinical practice. Am J Psychiatry. 2010 Sep;167(9):1125; author reply 1125-6.
Amen, D. G., Wu, J., George, N., & Newberg, A. (2020). Patterns of Regional Cerebral Blood Flow as a Function of Obesity in Adults. Journal of Alzheimer’s disease : JAD, 77(3), 1331–1337. PMC free article
Amen DG, Taylor DV, Ojala K, Kaur J, Willeumier K. (2013) Effects of brain-directed nutrients on cerebral blood flow and neuropsychological testing: a randomized, double-blind, placebo-controlled, crossover trial. Adv Mind Body Med. 2013 Spring;27(2):24-33.
Carrie Burdinski MS, an anatomy and physiology professor at Delta College, has an excellent 2 hour Youtube video on everything you need to know to understand the role of the autonomic nervous system in postural orthostatic tachycardia syndrome (POTS). Ms Burdinski does an excellent job of describing the physiology of non tachycardia symptoms of POTS like “brain fog” and loss of temperature control, both symptoms of Long Covid.
Ms Burdinski gave an interesting overview of different ways that genetics and epigenetics influence the regulation of the norepinephrine (noradrenaline) transporter that clears “used” noradrenaline from the the synaptic cleft. A quick title search of PubMed reveals the following
Mutations in the NET gene that result in a single amino acid substitution in the translated protein that affect the efficiency of noradrenaline / norepinephrine uptake.
Epigenetic methylation of the promoter of the NET gene that prevents translation of the gene into messenger RNA (mRNA)
Epigenetic micro RNA binding to the NET mRNA that prevents it from being translated into a protein.
Once the NET mRNA is translated into a protein, there are numerous “post translational” modifications that can regulate protein function. (Mandela and Ordway 2006)
Examples of regulating NET
These examples from the Mandela and Ordway review are pretty typical of protein regulation. We need to remember that the adrenergic receptors are also subject to regulation at the protein level.
Phosphates may be added to amino acids serine, threonine, and tyrosine by protein kinase C, casein kinase II, Ca2+ calmodulin kinase, and cAMP dependent protein kinase. The latter is particularly interesting because many heterotrimeric G proteins, of which the adrenergic receptors are a few of many, signal through an enzyme that makes cAMP.
A large number of neurotransmitters that bind to heterotrimeric G protein receptors
Protein phosphatases remove phosphates from serine, threonine, and tyrosine.
Insulin is known to decrease NET mRNA expression in locus coeruleus neurons of the rat
Atrial natriuretic factor (ANF) increases production of NET
Nerve growth factor decreases NET mRNA levels.
Nitric oxide may regulate NET by thiol nitrosation and/or cGMP dependent protein kinase.
We will not get into the dozens, if not hundreds, of pharmaceuticals that can regulate norepinephrine/noradrenaline release, reuptake, and binding to its many receptors. Ms Burdinsky was obviously frustrated with the myriad of pharmaceuticals not only to regulate these proteins up to mitigate the side effects.
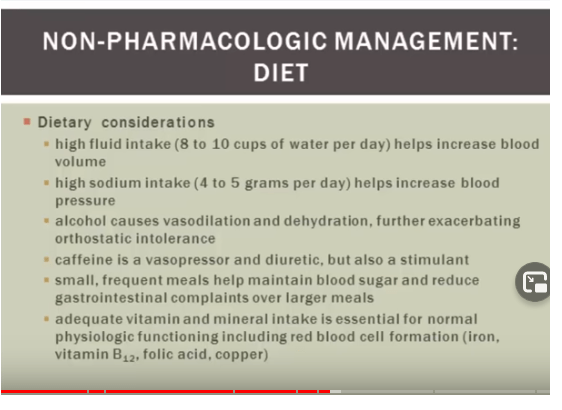
A screen shot of Ms Burdinski’s youtube lecture. This shot covers non pharmaceutical interventions for POTS.
Ms Burdinski went over the physiology behind each and every bullet point on this screen shot and why she thought these dietary interventions help POTS patients. The reasons behind copper were
Copper is needed for proper handling that we have covered in the ceruloplasmin post.
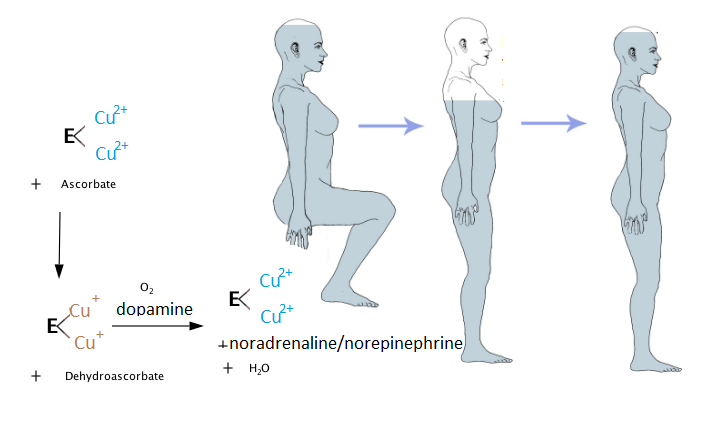
Ms Burdinski postulated that if the presynaptic neuron is that recycling used noradrenaline because of impaired reuptake by NET, it needs more copper for dopamine hydrolase, the enzyme that synthesizes noradrenaline from dopamine. If noradrenaline is not recycled, it just diffuses away from the synaptic cleft. Therefore the neuron needs to make more
Copper deficiency and autonomic dysfunction
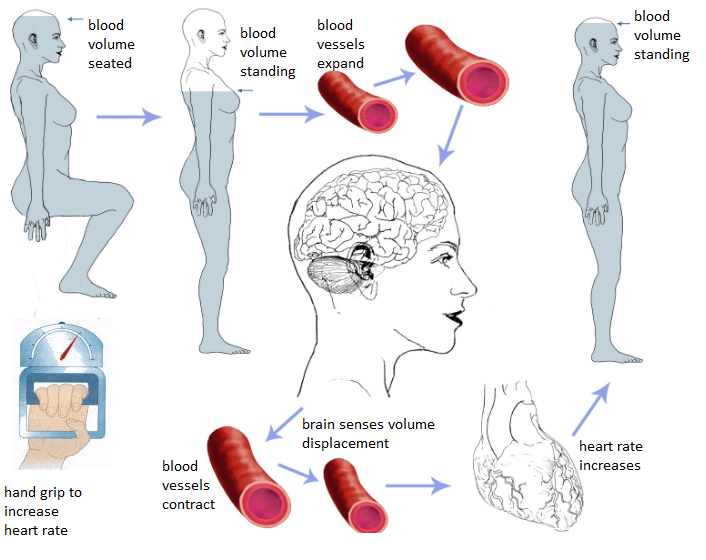
This 1988 study came from the United States Department of Agriculture, Agriculture Human Nutrition Research Center in Grand Forks, North Dakota. Lukaski and coworkers explored this link in female volunteers. This study seemed to start as a simple baroreceptor reflex investigation. When we are at rest, our brains get adequate blood flow. Upon standing gravity decreases the blood volume in our brains. This causes our blood vessels to contract.
When peripheral blood vessels do not properly contract when the woman stands, the brain continues to sense a volume displacement and the heart rate continues to increase. A hand grip exercise was used to increase the heart rate and divert just a small amount of the blood of the women to the exercising muscle.
The diets
Eight women, 18-36 years old, were monitored on four separate diets for a total of 135 days
basal, low diet copper 0.65 mg d -1 and adequate in ascorbic acid (90 mg d-l) 42 days
basal low copper + 1.5 g acid d -1 ascorbic acid for 42 days
basal + 0.8 mg d -1 copper, control normal copper, 14 days
basal +2 mg d –1 copper for 37 days, repletion.
Copper retention or chemical balance
Retention was calculated as the difference between intake and excretion in urine and feces. Menstrual and sweat loses were not considered.
At the end of each dietary period, fasting venous blood samples were obtained to determine biochemical indices of copper status.
Total plasma copper was determined by atomic absorption spectroscopy .
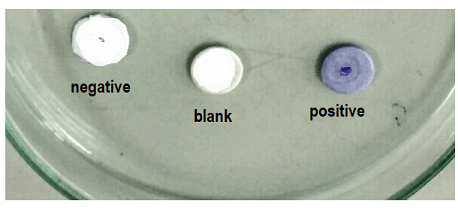
Ceruloplasmin enzymatic activity was assayed as a colorimetric p-phenylenediamine oxidase assay.
Ceruloplasmin content was measured by the radial immuno diffusion assay.
An image of the p-phenylenediamine oxidase assay.An image of the radial immuno diffusion assay. The bigger the circle the greater the activity.
Baroreceptor response
Autonomic cardiovascular function was assessed at the end of each dietary period.
Volunteers were tested in the post absorptive state after a 30-minute rest during which they were supine on a bed in a quiet room.
Variation in resting supine heart rate was determine over a three-minute period using the mean square successive differences of R-R intervals .
Orthostatic responses, upon arising form supine position and standing, were measured for heart rate and blood pressure.
Heart rate response was defined as the ratio of the R-R interval of the 30th to the 15th beat after standing.
Blood pressure was measured as each volunteer was supine and resting quietly and after one minute upon standing.
The hand grip exercise
Standing heart rate and blood pressure responses were determined before and during five minutes of sustained hand grip exercise with the dominant arm at 30% maximal voluntary contraction using a calibrated handgrip dynamometer.
Maximal voluntary contraction was determined at the end of each diet period.
Heart rate was recorded continuously using a multichannel electrocardiograph and standard limb leads.
Blood pressure was determined by auscultation on the inactive arm with diastolic pressure defined as the fourth phase Korotkov sound.
Results
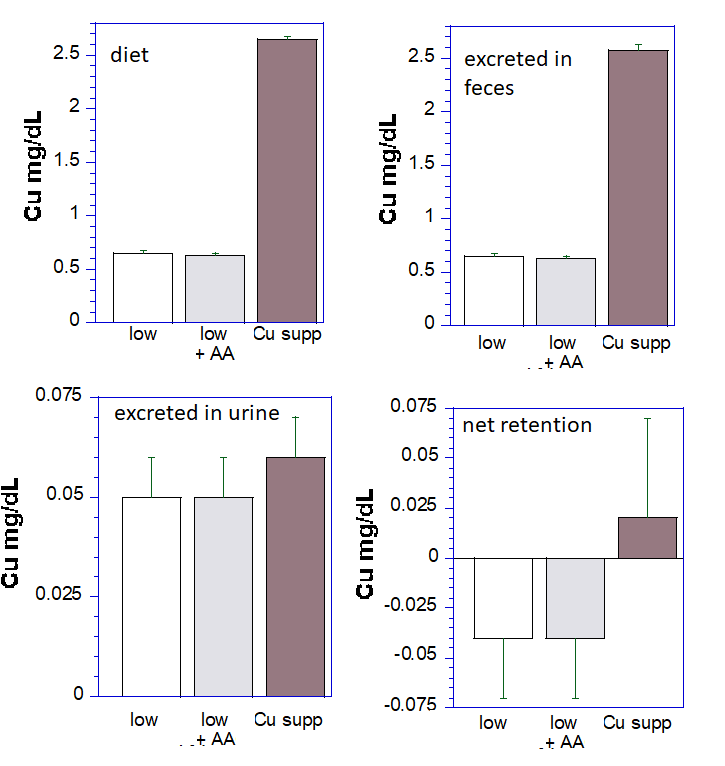
Most copper is excreted in the feces
These data are a graphical representation of Lukaski (1988) table 1. The data from the normal copper arm of the study were not collected, or presented in table 1.
Note that the copper supplemented diet has almost 5x the copper as the low copper diet. A remarkable observation in this study is that whether the copper is low or high, most of it is excreted in the feces. Virtually the same amount of copper is excreted in the urine. Retention of copper is higher in the copper supplemented arm of this study. Ascorbic acid (AA) had no influence on copper retention. What is not clear is if the large excretion of copper is due to failure to absorb it in the first place.
Dietary increases in copper and ceruloplasmin
The following graphs were reproduced from table 2 to emphasize the similarities and differences. Treatments different from the normal copper control at p<0.05 are indicated by “*â€. Variations of copper in these short term diets had no influence on plasma copper. All eight women spent some time in each group.
Data frp, table 2 of the Lukaski publication were graphed to emphasize the changes, and lack thereof
Concentrations of ceruloplasmin, as measured by radial immune diffusion, are in units of mg per liter of plasma. We can only assume that the authors used standards to calibrate the diffusion values. A ceruloplasmin reference range is 200-350 mg per liter. The low copper diet, with or without ascorbic acid (AA) decreased ceruloplasmin activity without decreasing the amount of protein. In fact, AA slightly increased the amount of ceruloplasmin protein in the plasma.
Ceruloplasmin enzymatic activity, in units of mg per liter, dropped (p<0.05) when the participants were on low copper diets with or without ascorbic acid (AA) supplementation. Copper supplementation to 2.65 mg per day did not increase the enzyme activity above what was observed when the participants over on 1.45 mg copper per day (Cu).
POTS spoiler, slight detour
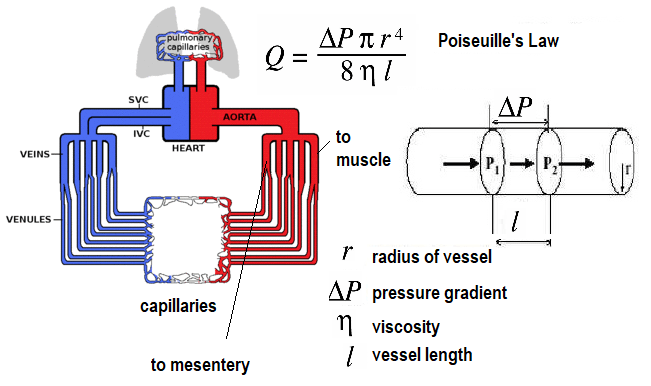
The spoiler alert, the authors reported no differences in the blood pressure responses from going to a supine position to standing. At the time of the study, the scientific community was becoming aware of the cardiovascular response to exercise. A short publication by Qumar and Read (1987) documented a decrease of blood flow to the mesenteric circulation to the small intestine in response to exercise. Many readers were told as children, “Don’t swim right after you eat lunch or you will get a stomach ache!”
If we are running from a dangerous situation, we’d want the blood flow (Q) to our gastrointestinal to decrease somewhat to allow more flow to our legs. When a vessel relaxes, the radius (r) becomes larger and flow increases. When the pressure gradient increases, flow increases. If all vessels were to simultaneously relax, blood flow have to drastically increase to keep the tissues oxygenated. Restricting the flow through some and increasing the flow through those arteries that supply muscles that are exercising means the cardiac output (flow) only has to increase a little bit.
Physical determinants of blood flow, Q. Note that small decreases in the radius of a blood vessel can result in very large decreases in flow. Lines point “to muscle” and “to mesentery.” Imagine another line that points “to brain” for the sake of POTS.
MAP may be estimated as the DP + 1/3 (SP-DP) where SP and DP are the systolic and diastolic blood pressures. It approximates the average pressure during the cardiac cycle. MAP is affected by factors such as:
Volume of blood pumped by the heart per minute (cardiac output, flow, Q)
Heart rate (beats per minute)
Blood pressure
Resistance to blood flow in the vessels
An increase or decrease in any of these factors can proportionately affect mean arterial pressure and bring corresponding consequences to the perfusion of major organs like the brain and kidneys.
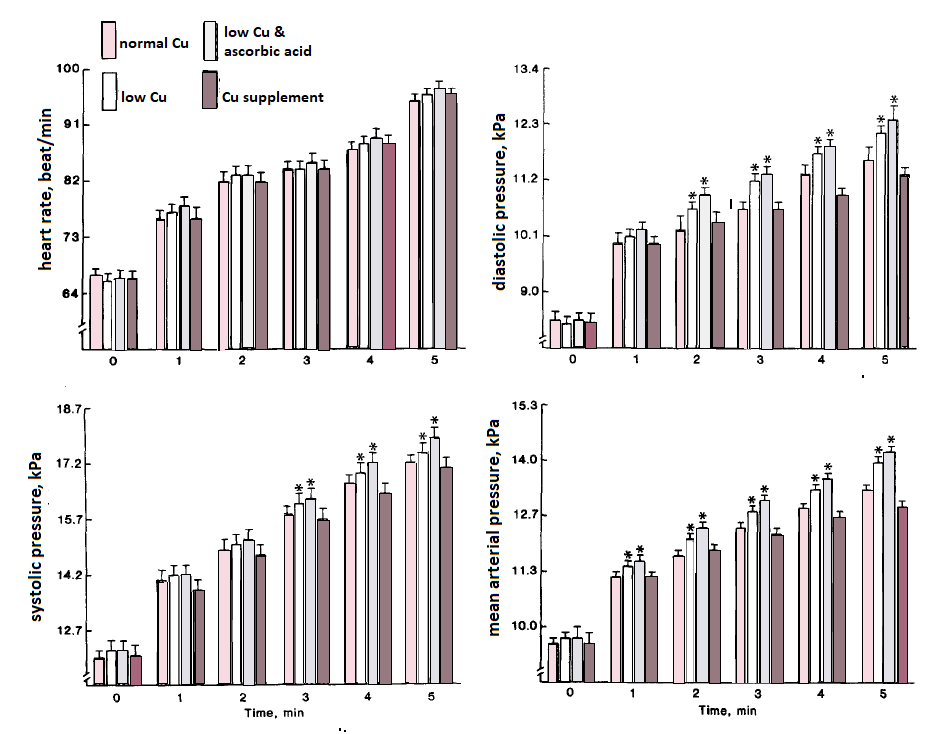
The heart rate was not different before the hand grip exercise started at time 0. The heart rate gradually increased during the 5 minutes of the exercise. The amount of copper made no difference. Overall significance of a copper effect (P<0.001) Maximum voluntary contraction was unaffected by copper.
The heart rate was not different before the hand grip exercise started at time 0. The heart rate gradually increased during the 5 minutes of the exercise. The amount of copper in the diet made no difference.
When the subjects were on low copper diets, their diastolic blood pressures increased more within 2 minutes (P<0.05) of hand grip exercise. (P<0.001) When the subjects were on low copper diets, their systolic blood pressures increased more within 3 minutes (P<0.05) of hand grip exercise.
Mean arterial pressure was noticeably elevated in the copper deficient subjects after only 1 minute of the hand grip exercise. Recall from Poiseuille’s Law that it is the pressure differential, ∆P, and resistance that drives flow.
Lukaski and coworkers discussed the possibility of vascular tone being altered by the impaired collagen cross linking enzyme lysyl oxidase. This group were experts in Cu/Zn superoxide dismutase 3 and angiotenin II activation of super oxide generator NADPH oxidase.
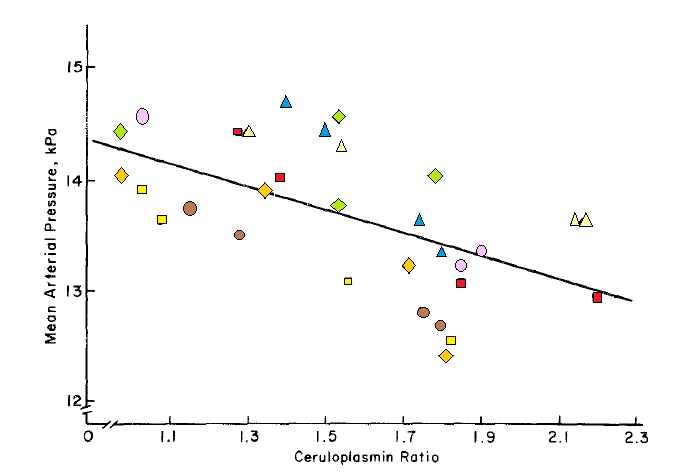
Ceruloplasmin loading of copper predicts MAP in response to exercise
A summary figure related the mean arterial pressure to the hand grip test to the “ceruloplasmin ratio.†This ratio is the enzymatic activity to the amount of the protein as measured by radial immune-diffusion. Each symbol represents an individual participant.
Liberty was taken to draw colored symbols over the poorly resolved black and white symbols in figure 2 of the Lukaski publication. “With the exception of one volunteer in whom this relationship was weak (r=-0.50), the individual relationships had correlation coefficients ranging from – 0.90 to – 0.99 (p<0.01). For the entire study sample, the ceruloplasmin ratio was a significant (p < 0.0004) predictor of mean arterial pressure at the end of the hand grip test.â€
The authors discussed the locus ceruleus as an integrator of afferent input with efferent output that control adrenergic cardiovascular reflexes (locus ceruleus-noradrenergic system or LC-NA system). This locus was also noted as being a copper enriched region of the brain. Blood pressure control during isometric hand grip exercise involves sympathetic (noradrenergic) afferent from skeletal muscle neurons. Lukaski and coworkers (1988) concluded that the involvement of copper required further study.
POTS and Long Covid?
The big question here is if POTS patients and those with Long Covid autonomic dysfunction are copper deficient. David Goldstein of the NIH has reviewed possible causes of POTS in Long Covid. Dr Goldstein gives a more in depth overview of some aspects of the ANS than covered in this post. He mentions autoimmunity. We have covered our research on NMDA repceptor suto antibodies in Long Covid in another post. Blitshteyn and Brook (2017) described a female patient who had received the HPV Cervavix vaccine who later developed POTS. This patient tested positive for anti-NMDA receptor antibodies, responded positively to immunomodulatory therapy, and had her symptoms come back when the therapy was discontinued. The CDC has addressed this association.
Given the prominence of ACE2 in the duodenum and small intestine, could copper absorption via Ctr1 be compromised in some Long Covid patients? Images are from ProteinAtlas.org
POTS and gluten sensitivity?
Copper deficiency in celiac disease has been addressed elsewhere. Are POTS patients more likely to have self reported gluten intolerance or bonefid celiac disease? Hugo Penny and coworkers (2016) of the Royal Hallamshire Hospital in Sheffield, UK surveyed 100 POTS patients. Four of the 100 POTS patients had serologically and biopsy proven celiac disease. Gluten sensitivity was reported in 42% of these 100 POTS patients versus 19% of the control population.
References
Blitshteyn S, Brook J. (2017) Postural tachycardia syndrome (POTS) with anti-NMDA receptor antibodies after human papillomavirus vaccination. Immunol Res. 2017 Feb;65(1):282-284.
Goldstein D. S. (2021). The possible association between COVID-19 and postural tachycardia syndrome. Heart rhythm, 18(4), 508–509.
Hoggard N, Hadjivassiliou M, West JN, Sanders DS. Is there a relationship between gluten sensitivity and postural tachycardia syndrome? Eur J Gastroenterol Hepatol. 2016 Dec;28(12):1383-1387
Lukaski HC, Klevay LM, Milne DB.(1988) Effects of dietary copper on human autonomic cardiovascular function. Eur J Appl Physiol Occup Physiol. 58(1-2):74-80.
Mandela P, Ordway GA. (2006) The norepinephrine transporter and its regulation. J Neurochem. 2006 Apr;97(2):310-33. doi: 10.1111/j.1471-4159.2006.03717.x. Epub 2006 Mar 15. PMID: 16539676 Free article.
Neselioglu S, Ergin M, Erel O. (2017) A New Kinetic, Automated Assay to Determine the Ferroxidase Activity of Ceruloplasmin. Anal Sci.33(12):1339-1344.
Qamar MI, Read AE.(1987)Effects of exercise on mesenteric blood flow in man. Gut. 28(5):583-7.
In another post the role of Cu/Zn SOD3 in mitigating blood pressure changes was introduced. Cu/Zn SOD3 removes superoxide before it can react with the vasodilating agent nitric oxide. Early studies showed that politicosanol increased the vasodilation in response to the NO releasing agent nitroprusside [1]
A group of Korean investigators became interested in politicosanol, a family of aliphatic alcohols of 24-34 carbons [2]. Policosanol is a byproduct of sugar cane wax. The alcohol ethanol has only two carbons. Dodecanol, also called lauryl alcohol, has only 12 carbons. The idea was to recruit participants who were pre- hypertension and divide them into three groups. Sometimes scientists and medical sorts like to look at the images first. The following are images available to the public from the link associated with reference [2].
Figure 1 from reference [2] Design of study and participants. Inclusion criteria were normolipidemic, normoglycemic, and healthy subjects who had prehypertension (systolic 130–139 mmHg, diastolic 80–89 mmHg). M: Male; F: Female.Data are expressed as mean ± SD. * p < 0.05 vs. week 0; ** p < 0.01 vs. week 0; *** p < 0.001 vs. week 0 in each group. M: male; F: Female; BP: blood pressure; SD: Standard deviation
In just 8 weeks participants taking 20 mg policosanol daily saw improvements in aortic and peripheral blood pressure. These participants seemed to have lost a little bit of subcutaneous and visceral fat.
Data are expressed as mean ± SD. * p < 0.05 vs. week 0; ** p < 0.01 vs. week 0; *** p < 0.001 vs. week 0 in each group. [2]From reference [2] Figure 2. Change of peripheral blood pressures (SBP and DBP) during 12-week consumption of policosanol groups and placebo group from repeated measurement ANOVA. Data are expressed as mean ± SEM. SBP: systolic BP; DBP: diastolic BP; SEM: standard error of mean. Follow the link below to view the table of ANOVA results.Data are expressed as mean ± SD, * p < 0.05 vs. week 0; ** p < 0.001 vs. week 0 in each group. TC, total cholesterol; TG, triglyceride; HDL-C, High-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol.
The authors speculated that the policosanol lowers blood pressure by increasing the fraction of high density lipo protein (HDL). According the the US CDC HDL is responsible for ferrying excess cholesterol back to the liver where it can be excreted. Indeed, Park and coworkers found an inverse correlation between blood pressure and HDL (see supplemental data of reference [2]). In a previous clinical trial the same group demonstrated that Cuban policosanol inhibited inhibited cholesterol ester transferase protein (CETP). [3]
Park, H. J., Yadav, D., Jeong, D. J., Kim, S. J., Bae, M. A., Kim, J. R., & Cho, K. H. (2019). Short-Term Consumption of Cuban Policosanol Lowers Aortic and Peripheral Blood Pressure and Ameliorates Serum Lipid Parameters in Healthy Korean Participants: Randomized, Double-Blinded, and Placebo-Controlled Study. International journal of environmental research and public health, 16(5), 809. https://doi.org/10.3390/ijerph16050809 PMC free article
Kim JY, Kim SM, Kim SJ, Lee EY, Kim JR, Cho KH. Consumption of policosanol enhances HDL functionality via CETP inhibition and reduces blood pressure and visceral fat in young and middle-aged subjects. Int J Mol Med. 2017 Apr;39(4):889-899. doi: 10.3892/ijmm.2017.2907. Epub 2017 Feb 24. PMC free article
This information was first posted back in May of 2020 during the Covid-19 lock down. The makers of cuprous nicotinic acid paid BL of BDLbiochem.com to post this information. We were going over data from a clinical trial conducted in 2014 by what was then called KGK Synergy. The medical scientists came up with a perfectly rational hypothesis as to how the copper might relieve pain that cuprous nicotinic acid customers described. We didn’t see that much of acute pain relief. This post explores the role of copper in flood flow in muscles. Upon reviewing the literature I came up with the hypothesis that chronic muscle discomfort might arise from poor blood flow. This is where copper and nicotinic acid might come in. If you use skin creams to relieve muscle pain you might want to check out Jefro’s Botanicals. I’ve been doing terpene research as a hobby and looked into the composition of Gaming Balm. This stuff has the potential to be better than Bengay. Let’s get back to the original post!
Blood flow in muscles
KGK Synergize “In addition to the possible analgesic effects facilitated by NMDA receptor inhibition, both copper and nicotinic acid are thought to support mitochondrial function by improving cellular respiration, thus increasing ATP production (1-3). Studies investigating muscle pain in relation to occupational work have demonstrated that sore muscle displays changes in structure indicating mitochondrial disturbances and reduced oxygenation (4,5). A recent study found that nicotinic acid treatment improved overall cellular respiration and was able to reverse deleterious effects on crucial cellular functions that are impaired in mitochondrial respiratory chain diseases (2).  Copper is required within the mitochondria for assembly of the enzymes cytochrome c oxidase (CcO) and superoxide dismutase (Sod1). Decreased rates of electron transfer observed in dysfunctional mitochondria are most often due to diminished activity of CcO (6).  Reports have shown that supplementation of copper can reverse CcO deficiency, thus increasing production of ATP (1,7,8). The enhancement of mitochondrial function by copper and nicotinic acid may also act to prevent the structural changes in muscle that are associated with pain.
Both copper and nicotinic acid on their own are essential for many biological processes and have been used as therapeutic agents. Copper is necessary for the activity of several key enzymes in the cell, primarily in the mitochondria where it plays a role in energy metabolism and protection against oxidative stress (1,9,10). Copper complexes can also modulate copper homeostasis in the brain, resulting in protective effects in several models of neurodegeneration (9). Copper is also important in synaptic function, specifically regarding axonal targeting and synaptogenesis (10,12).
Nicotinic acid, also known as niacin or vitamin B3, plays a role in production of energy, signal transduction, regulation of gene expression, and is involved in the synthetic pathway of lipids (13,15). It has long been used as broad-spectrum lipid drug, as it lowers the levels of all atherogenic lipoproteins and raises the levels of the protective HDL lipoproteins (13). Recently, nicotinic acid has been shown to partially restore normal functioning in cells taken from patients with mitochondrial diseases by normalizing signaling activity and improving overall cellular respiration(2). “
BDLbiochem …. KGK did a very impressive job of summarizing the peer reviewed literature. The participates with neuro muscular pain that they were able to recruit added a new out look opened new possibilities. One thing that caught my attention was the large number of participants in the study that had neck and shoulder discomfort. Trapezius muscle discomfort is very common among office workers. Another thing that caught my attention was that many of the participants started the study dehydrated. Dehydration can lead to release of angiotensin II. Angiotensin II not only causes blood vessels to contract but also activates NADPH oxidase to produce a reactive oxygen species superoxide. As a general background (8),
Acetylcholine binds to receptors on the membranes of endothelial cells.
Activated phospholipase C cleaves IP3 from its parent phospholipid.
IP3 causes the release of Ca2+ from intracellular stores.
Ca2+ binds to calmodulin.
Ca2+CaM activates nitric oxide synthase, which produces nitric oxide.
Nitric oxide binds to guanylate cyclase in smooth muscle of blood vessels.
Guanylate cyclase converts GTP to cyclic GMP.
cGMP activates protein kinase G.
Protein kinase G phosphorylates proteins that cause smooth muscle to relax.
Nitric oxide (NO) controls blood flow (8) to skeletal muscles and to every other organ. As an aside, NO also controls gut muscle relaxation (8).
If superoxide (O2.-) is present, from neutrophils from the innate immune system, also produces O2.- which reacts with nitric oxide (NO) to form peroxynitrite (ONOO–) before NO. can cause blood vessels to dilate.
Two main ways of preventing nitric oxide (NO) from relaxing blood vessels that vascularize skeletal muscle A. The angiotensin II receptor activates NADPH oxidase that produces pueroxide ( O2.-). B. Neutrophils also produce O2.-. (16)
Dietary Copper matters
Cu/Zn is important
Dietary copper influences acetylcholine induced vasorelaxation in the rat (17). , Arteriole dilation in response to increasing concentrations of acetylcholine (10-7 to 10-4 ) was measured in vivo in the cremaster muscle microcirculation for each dietary copper group:
Deficient
Marginal
Adequate
Schuschke and coworkers (17) used liver copper concentration and aortic and erythrocyte Cu/Zn-SOD activity as indices of systemic copper status. When Cu increased from 0 μg per gram dry weight in the liver an exponential increase in 10-5 M acetylcholine (Ach) induced vasodilation was seen. This suggested that concentrations below 5 μg copper per dry liver weight results in attenuated vasodilation.
Copper deficiency prevents vasodilation
An earlier study from the same group, using a similar model (18), suggested that Cu/Zn SOD3 protected nitric oxide’s role as a vasodilator by scavenging superoxide before it could react with nitric oxide. Cremaster arteriole endothelial intracellular Ca2+ stimulated by 10-6 M Ach was significantly inhibited in the arterioles from Cu deficient rats. The inhibition of Ca2+ and vasodilation was accompanied by a depression of vascular Cu/Zn-SOD activity and an increase in plasma peroxynitrite activity. The authors suggested oxidative damage to proteins involved in Ca2+ signaling (18).
Copper protects NO
Another study from the Schuschke group (19) compared nitric oxide production from lung microvascular endothelial cells made copper deficient with a chelator with copper adequate endothelial cells. A fluorescent NO indicator showed NO significantly decreased in the copper deficient endothelial cells under basal as well as acetylcholine stimulated conditions (19). This group found he same thing in the cremator muscle arterioles from the copper deficient versus copper sufficient rats (19). They used kidney and liver concentrations of copper to verify deficiency. Blood plasma not considered a reliable indicator of copper status.
A different group examined the relationship between angiotensin II induced superoxide production increases in blood pressure and its mitigation by Menke’s (MNK, aka ATP7A) copper transporter (Qin 2008).
It’s also about copper (+1) loading
A different group examined the relationship between angiotensin II induced superoxide production increases in blood pressure and its mitigation by Menke’s (MNK, aka ATP7A) copper transporter (20).
In the model developed in this study Angiotensin II causes the extracellular SOD3 to associate with ATP7A (MNK) in the Golgi for Cu loading before it is secreted (Qin 2008). The end result is that superoxide is scavenged before it can react with NO. The blood work suggested that patients in the Mitosynergy/KGK Synergize study might have started out with high angiotensin II, an activator of NADPH oxidase that produces superoxide.
Are changes in muscle microcirculation involved in chronic muscle discomfort?
Many of the participants in the KGK study had chronic shoulder pain, presumably in the trapezius. This is a common site of pain for those who spend a lot of time at the key board. The following is a brief review of the literature involving vascular changes in trapezius muscle pain. This image was compiled for the reader to conceptualize the trapezius muscle discomfort from repetitive key boarding.
Office workers and other who spend a lot of time at a key board may experience trapezius muscle discomfort
Right handed female office workers, with and without chronic pain in the trapezius muscle, were asked to perform tasks such as typing and mousing. The main finding of this study was that 1 h of combined workstation tasks resulted in decreased oxygen saturation and blood flow in the upper, middle, and lower trapezius (21). Oxygen saturation was significantly lower in the trapezius myalgia cases compared to the control group (p = 0.027). Blood flow of the upper trapezius on the right side was significantly lower than the blood flow on the left side (p = 0.026).
Blood flow in female and male patients diagnosed with trapezius myalgia were compared with healthy controls. The right and left trapezius muscles of all individuals were examined simultaneously with laser-Doppler flowmetry (LDF) and surface EMG during a fatiguing series of step-wise-increased contractions. Duration was for 1 min with 1 min rest in between. (22). Trapezius myalgia patients showed significantly lower blood flow in the painful side with low contraction frequencies.
Another office worker trapezius myalgia study showed pain in the active side correlated positively with blood flux in the pain-afflicted subjects and negatively in the reference group. This study showed that pain is associated with trapezius vasodilation but not with muscle activity (23). This study came to the conclusion that interaction between blood vessels and nociceptors may be important in the activation of muscle nociceptors in people with chronic shoulder and neck pain (23).
Metabolic substances and trapezius blood flow were measured in female office workers with and without chronic pain over the course of an eight hour day (Larsson 2008). Increased concentrations of glutamate and pyruvate were seen in the pain group compared to the controls. Increased blood flow was seen in the trapezius pain group (24).
Office workers with trapezius myalgia were compared with pain free office workers performing repetitive “peg board†and a stress task. Insufficient muscle blood flow and oxygenation were proposed to account for the higher lactate, pyruvate and pain responses among myalgia suffers versus controls (25).
A study sought to compare blood flow and oxygen saturation with trapezius and extensor carpi radius muscle fatigue in workers with and without work related muscle pain (26). While fatigue in response to repetitive tasks occurred earlier in the pain group, no changes were seen in hemodynamics and blood oxygen saturation between the control and he pain group (26). These authors that a central, rather than a peripheral, mechanism accounted for the early fatigue.
Conclusion
Much information exists on the role of nitric oxide, blood flow, and discomfort in muscle groups that do not receive adequate blood flow. The role of copper supplements in mitigating muscle discomfort due to inadequate blood flow deserves follow up in a better controlled study. See study results for tasks that became less uncomfortable with the group on Cu(I)NA2.
References
Salviati L, Hernandez-Rosa E, Walker WF et al. Copper supplementation restores cytochrome c oxidase activity in cultured cells from patients with SCO2 mutations. Biochem J 2002;363:321-7.
Zhang Z, Tsukikawa M, Peng M et al. Primary respiratory chain disease causes tissue-specific dysregulation of the global transcriptome and nutrient-sensing signaling network. PLoS One 2013;8:e69282.
DiMauro S, Schon EA. Mitochondrial respiratory-chain diseases. N Engl J Med 2003;348:2656-68.
Gracely RH, Petzke F, Wolf JM, Clauw DJ. Functional magnetic resonance imaging evidence of augmented pain processing in fibromyalgia. Arthritis Rheum 2002;46:1333-43.
Cook DB, Lange G, Ciccone DS, Liu WC, Steffener J, Natelson BH. Functional imaging of pain in patients with primary fibromyalgia. J Rheumatol 2004;31:364-78.
Navarro A, Boveris A. The mitochondrial energy transduction system and the aging process. Am J Physiol Cell Physiol 2007;292:C670-C686.
Cobine PA, Pierrel F, Bestwick ML, Winge DR. Mitochondrial matrix copper complex used in metallation of cytochrome oxidase and superoxide dismutase. J Biol Chem 2006;281:36552-9.
Jaksch M, Paret C, Stucka R et al. Cytochrome c oxidase deficiency due to mutations in SCO2, encoding a mitochondrial copper-binding protein, is rescued by copper in human myoblasts. Hum Mol Genet 2001;10:3025-35
Duncan C, White AR. Copper complexes as therapeutic agents. Metallomics 2012;4:127-38.
Leary SC, Winge DR, Cobine PA. “Pulling the plug” on cellular copper: the role of mitochondria in copper export. Biochim Biophys Acta 2009;1793:146-53.
Olsen NJ, Park JH. Skeletal muscle abnormalities in patients with fibromyalgia. Am J Med Sci 1998;315:351-8.
Bengtsson A, Henriksson KG. The muscle in fibromyalgia–a review of Swedish studies. J Rheumatol Suppl 1989;19:144-9.
Carlson LA. Nicotinic acid: the broad-spectrum lipid drug. A 50th anniversary review. J Intern Med 2005;258:94-114.
Depeint F, Bruce WR, Shangari N, Mehta R, O’Brien PJ. Mitochondrial function and toxicity: role of B vitamins on the one-carbon transfer pathways. Chem Biol Interact 2006;163:113-32.
Hageman GJ, Stierum RH. Niacin, poly(ADP-ribose) polymerase-1 and genomic stability. Mutat Res 2001;475:45-56.
Wimalawansa S J. Nitric oxide: new evidence for novel therapeutic indications Expert Opinion on Pharmacotherapy 2008. 9(11):1935-1954 Link
Schuschke DA, Percival SS, Saari JT, Miller FN.(1999) Relationship between dietary copper concentration and acetylcholine-induced vasodilation in the microcirculation of rats. Biofactors. 10(4):321-7.
Schuschke DA, Saari JT, Miller FN.(1995)A role for dietary copper in nitric oxide-mediated vasodilation.Microcirculation. 1995 Dec;2(4):371-6.
Falcone JC, Lominadze D, Johnson WT, Schuschke DA.(2008) Endothelial cell-derived nitric oxide mobilization is attenuated in copper-deficient rats. Appl Physiol Nutr Metab. 33(6):1073-8.
Qin Z, Gongora MC, Ozumi K, Itoh S, Akram K, Ushio-Fukai M, Harrison DG, Fukai T. (2008) Role of Menkes ATPase in angiotensin II-induced hypertension: a key modulator for extracellular superoxide dismutase function. Hypertension.52(5):945-51.
Cagnie B, Dhooge F, Van Akeleyen J, Cools A, Cambier D, Danneels L.(2012) Changes in microcirculation of the trapezius muscle during a prolonged computer task. Eur J Appl Physiol.112(9):3305-12
Larsson R, Oberg PA, Larsson SE(1999) Changes of trapezius muscle blood flow and electromyography in chronic neck pain due to trapezius myalgia. Pain. 79(1):45-50.
Strøm V, Røe C, Knardahl S.(2009) Work-induced pain, trapezius blood flux, and muscle activity in workers with chronic shoulder and neck pain. Pain.144(1-2):147-55.
Larsson B, Rosendal L, Kristiansen J, Sjøgaard G, Søgaard K, Ghafouri B, Abdiu A, Kjaer M, Gerdle B.(2008) Responses of algesic and metabolic substances to 8 h of repetitive manual work in myalgic human trapezius muscle. Pain. 140(3):479-90.
Sjøgaard G1, Rosendal L, Kristiansen J, Blangsted AK, Skotte J, Larsson B, Gerdle B, Saltin B, Søgaard K.(2009) Muscle oxygenation and glycolysis in females with trapezius myalgia during stress and repetitive work using microdialysis and NIRS. Eur J Appl Physiol. 108(4):657-69
Elcadi GH, Forsman M, Hallman DM, Aasa U, Fahlstrom M, Crenshaw AG3.(2014) Oxygenation and hemodynamics do not underlie early muscle fatigue for patients with work-related muscle pain. PLoS One. 2014 Apr 22;9(4):e95582