Neuro PASC, after three weeks
It was common for patients hospitalized to develop encephalitis, an inflammation of the brain. It makes sense that these patients would develop long term neurological symptoms of what is now being called post acute sequelae of Covid-19. (PASC) Some Covid-19 patients who were never hospitalized, and who only experienced mild symptoms, have gone on to develop nuero-PASC as well.
Methods
A multi-center group of investigators recruited hospitalized, post hospitalized, and non-hospitalized patients with confirmed diagnosis of COVID-19 with neurologic symptoms in addition to healthy control (HC) subjects. Their blood plasma was assayed for three proteins
- neurofilament light chain (pNfL), a marker for injured neurons
- plasma glial fibrillary acidic protein (pGFAP), a marker for astrocytes, nurse cells of neurons
- SARS-CoV-2 Nucleocapsid antigen (pN Ag)
Neurofilament (neurons), GFAP (astrocytes), and the ratio
This figure looks at two proteins from dead brain cells in the blood. Naturally there are more of these brain cell proteins in older individuals than in the young. When the ratio of GFAP to neurofilament is high, the pathology is more on the astrocyte side of things.
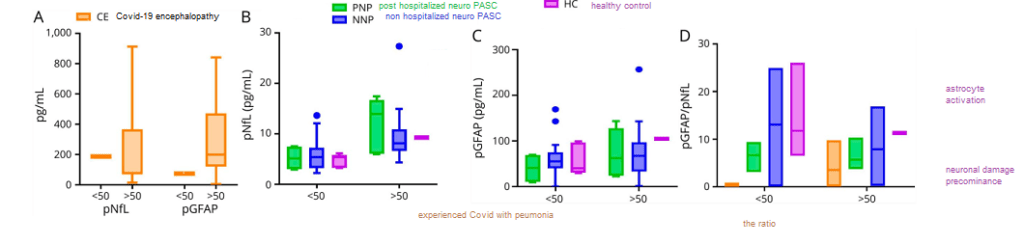
These data indicate the noise due to the age of the patient that will contribute to any serum protein or the ratio thereof.
A Covid protein in the blood three weeks after the first sign of symptoms

Age notwithstanding, the Covid-19 nucleocapsid was only seen in one of the PASC patients, and that patient was was never hospitalized. The really perplexing thing about these data is (1) the percentage of neuro-PASC patients that experienced most of the symptoms and (2) when there was a difference between the post hospitalized and never hospitalized patients, the never hospitalized patients fared the worse.
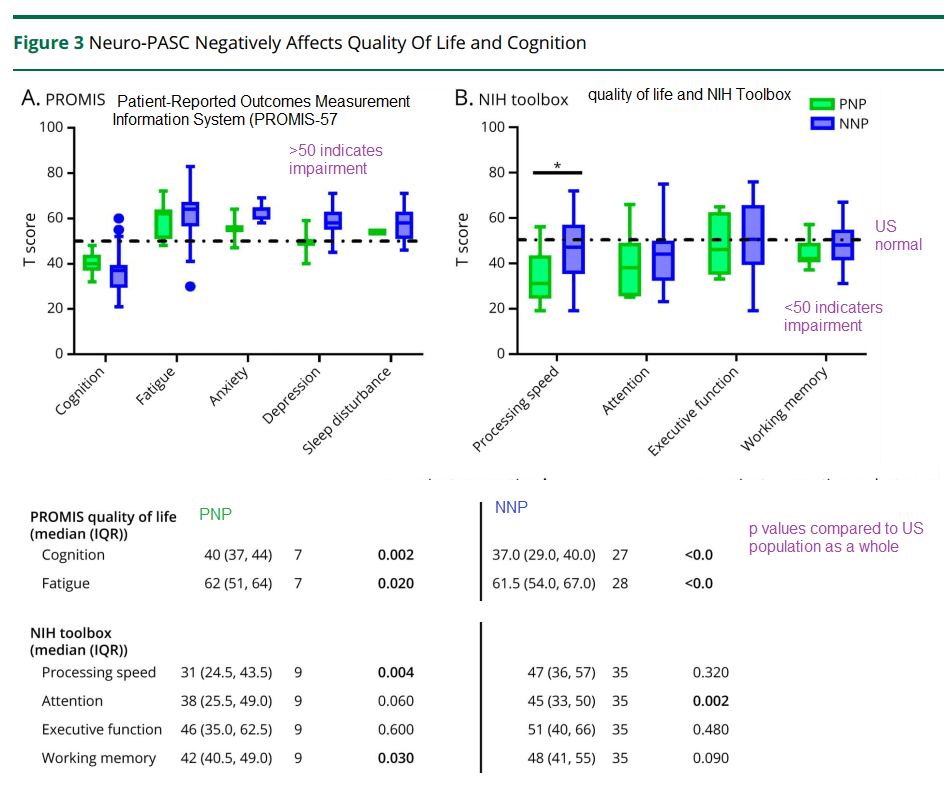
Neurological tests three weeks later
The patients were given these tests three weeks after the onset of acute Covid-19 symptoms. They are still impaired compared to the US average. This post is not getting into the analysis controls used to guarantee the integrity of the data.
Hanson and coworkers also performed some regression analysis of depression and anxiety symptoms as a function of the ratio of GFAP to neurofilament…
- When stratified by age, those patients with depression/anxiety were more likely to have a high GFAP/neurofilament ratio. This was true for both those over 50 years old and those less than 50 years old. (p<0.05)
- A positive correlation was seen in the Promis T score for anxiety as a function of the GFAP/neurofilament immuno reactivity in the plasma. (p=0.03) R2 was only 0.041.
- There was no correlation between the Promis T score for depression and the plasma immuno reactivity GFAP/neurofilament ratio.
The amazing thing in this study is how many patients are compromised three weeks after the initial onset of Covid-19 symptoms. The hints of astrocyte dysfunction are in keeping with the Goetzl findings described in another post.
A yet to be peer reviewed study from Brazil:
A Brazilian group has demonstrated the presentation of the SARS-Cov2 virus in astrocytes in the brains of deceased Covid-19 patients. They further demonstrated the ability of SARS-Cov2 to infect astrocytes using NRP1 as an alternative receptor to ACE2. [1] The Brazilians produced astrocytes from neuronal stem cells, infected them with SARS-CoV2, and used mass spectrometry to measure the levels of key neurotransmitters,
Figure 7 Sea Horse and related metabolic data

High resolution mass spectrometry was used to compute the violin plots shown of the end product of terminal glycolysis, lactate, and the intermediate before entry into the TCA cycle, pyruvate. TCA cycle intermediates were not different between mock and CoV2 infected astrocytes. (Figure 10 supp, not shown)

Cellular respiration of mock and CoV2 infected astrocytes was measured in a Sea Horse respirometer. Basal respiration, ATP production, and the reserve capacity were not significantly different in the infected astrocytes compared to the mock infected astrocytes. The proton leak, maximum respiration, and non-mitochondrial oxygen consumption were, however, greater in the CoV2 infected astrocytes. We’ve discussed Covid proteins binding to Complex I proteins in a previous post. Complex I might be the source of non (normal) mitochondrial oxygen consumption the Brazilians referred to.
In summary..
These data support astrocyte involvement in Long Coivd/ PASC. How do we address this in a clinical trial? Do monocytes and CD8+ cytotoxic T cells migrate into the brain?
References
- Hanson, B. A., Visvabharathy, L., Ali, S. T., Kang, A. K., Patel, T. R., Clark, J. R., Lim, P. H., Orban, Z. S., Hwang, S. S., Mattoon, D., Batra, A., Liotta, E. M., & Koralnik, I. J. (2022). Plasma Biomarkers of Neuropathogenesis in Hospitalized Patients With COVID-19 and Those With Postacute Sequelae of SARS-CoV-2 Infection. Neurology(R) neuroimmunology & neuroinflammation, 9(3), e1151. PMC free article
- https://www.medrxiv.org/content/10.1101/2020.10.09.20207464v5
Leave a Reply