The Individualized Neuromuscular Quality of Life
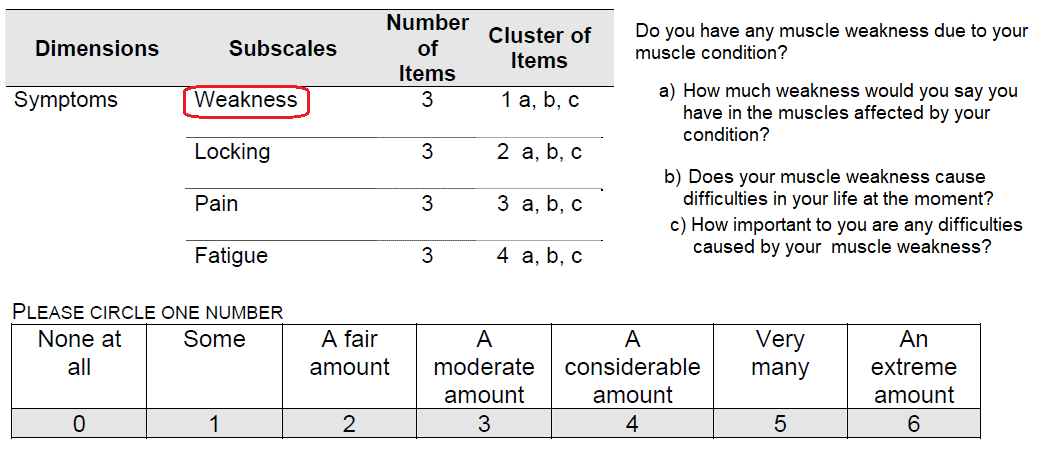
KGK Synergize, “The primary objective of this study was to determine the effect of treatment on quality of life using the INQoL. The INQoL is a muscle-disease specific QoL questionnaire devised of 45 questions sub-divided into 12 sub-domains. Four of the sub-domains focus on the impact of muscle disease symptoms such as weakness, locking, pain, and fatigue, 5 look at the impact of the disease on various life domains such as activities, independence, social relationships, emotions and body image, and the treatment effects sub-domain focuses on the positive and negative effects of perceived treatment and expected treatment effects. A final section looks at the overall effect of the condition on QoL which is a compilation of scores on questions from the activities, independence, social relationships, emotions and body image subscores. This questionnaire has previously been validated in European and American muscle disease patient populationsâ€
KGK Synergize “In conclusion, although there were no significant differences between participants supplemented with Cunermuspir (Cu(I)NA2)or placebo in the Quality of Life assessed by the Individualized Neuromuscular Quality of Life Questionnaire, participants on Cunermuspir reported a significant 34% reduction in Fatigue, 26% improvement in muscle locking, and a 15% reduction in pain from baseline to end of treatment. In contrast, subjects on placebo reported a 12% increase in Fatigue. It is noteworthy, that participants on Cunermuspir (Cu(I)NA2) showed a 46% improvement in Fatigue over participants on placebo. It is possible that the within group significance in the INQoL Quality of Life may have reached between group significance with a larger sample size and a longer period of supplementation.
Let us take a look at the symptoms module with four subdomains
KGK Synergize “In conclusion, although there were no significant differences between participants supplemented with Cunermuspir or placebo in the Quality of Life assessed by the Individualized Neuromuscular Quality of Life Questionnaire, participants on Cunermuspir reported a significant 34% reduction in Fatigue, 26% improvement in muscle locking, and a 15% reduction in pain from baseline to end of treatment. In contrast, subjects on placebo reported a 12% increase in Fatigue. It is noteworthy, that participants on Cunermuspir showed a 46% improvement in Fatigue over participants on placebo. It is possible that the within group significance in the INQoL Quality of Life may have reached between group significance with a larger sample size and a longer period of supplementation.
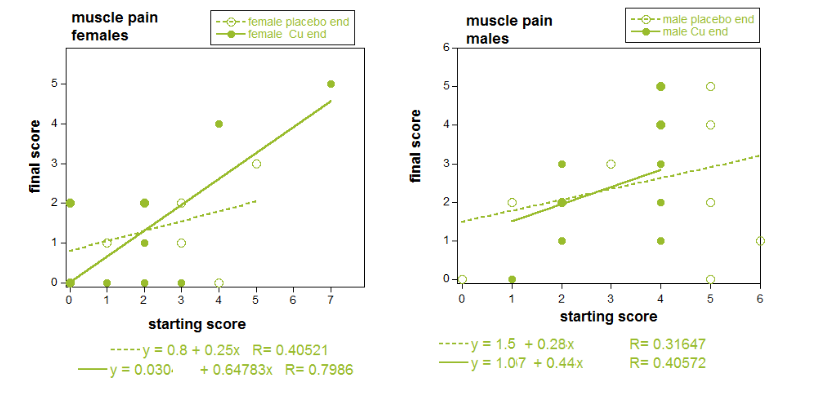
The Mitosynergy adage that those that start the copper in a bad state improve the most did not seem to hold true for INQoL reported fatigue.  The final scores in the INQoL questionnaire were plotted as a function of starting scores. The slopes of these lines were calculated using the Kaleidograph software (Senergy Software Inc).
Fatigue
One participant had neuromuscular pain in right thigh and calf. Another participant had pain the right shoulder and arm. Sciatica was a common complaint. One participant had “muscle aches and stabbing/shooting pains in the upper body.†A major flaw in my opinion is that the questionnaire never defined “fatigue. “Muscle fatigue†can be defined as the decline in ability of a muscle to generate force. This decline may be due to a defect in the nerve that tells the muscle to contract and or to a defect tin the contractile apparatus in the muscle fiber itself. We have no way of knowing how the participants defined pain when they answered the questions.  It was likely to have been different from the physiologist contributor to Wikipedia. The task in which the “fatigue†was experienced was also never defined. Did the person experiencing pain in the right calf and thigh have muscles that simply ceased to contract after prolonged walks? If the copper helped, did the walks last longer before the fatigue set in?
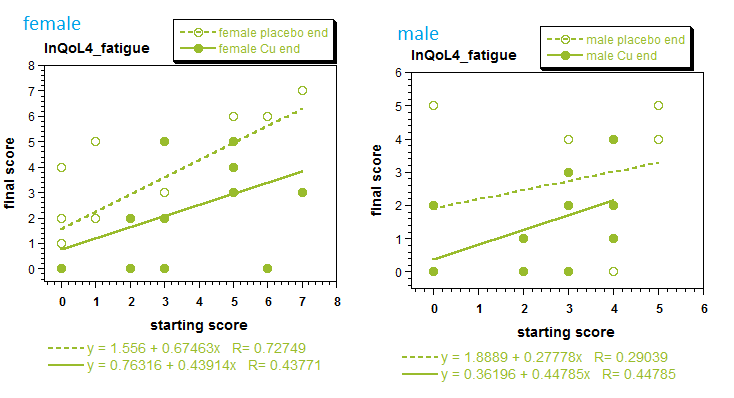
These data, with a very diverse “neuromuscular pain” study group, represent an unbiased sampling of what Mitosynergy has observed anecdotally. Two of the three males who started the study with a fatigue score of 4 improved considerably. Three of the females on Cu(I) started the study with some level of “fatigue” ended the study with a fatigue score of 0. Many in the placebo group had less fatigue at the end of the study.
Fatigue is listed as a symptom of COVID-19 in some studies and reviews (Li 2020) and not others (Lechien 2020). The ACE2 enzyme/COID-19 receptor is expressed in skeletal muscle and the adrenal gland (Li 2020). Takeshita and coauthors (2020) compared grip strength and running distance of wild type mice and mice in which the gene that codes for ACE2 had been knocked out. Lack of functional ACE2 enzyme decreased grip strength and running distance. Some of this was reversed by injection of he ACE2 product, angiotensin 1-7. It would be interesting to quantify COVID-19 related fatigue in some sort of metric like “grip strength” and/or amount of walking before feeling tired.
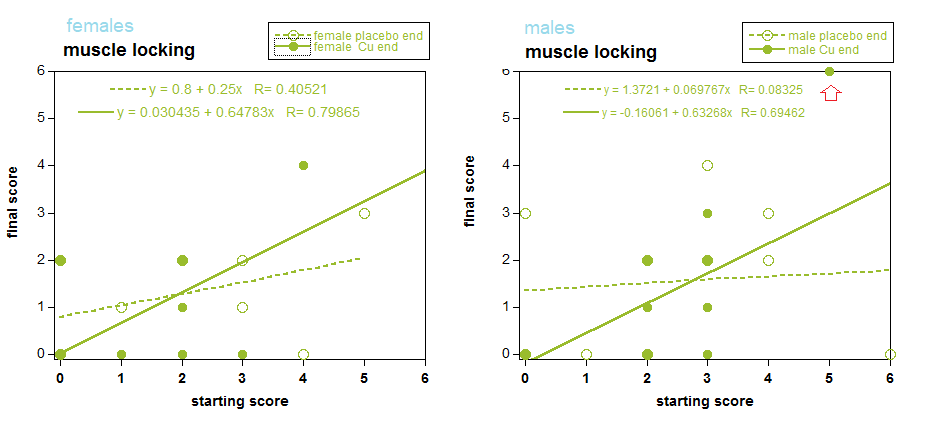
Muscle locking
It is not certain if muscle locking is the same thing as muscle cramps, a site created by the WikiMecine Protect. Muscle cramps are usually defined by involuntary contraction of skeletal or smooth muscle. They may originate from any component of actin-myosin cross bridge cycling from reuptake of calcium by the sarcoplasmic reticulum to generation of ATP that is needed to release rigor states.
Pain
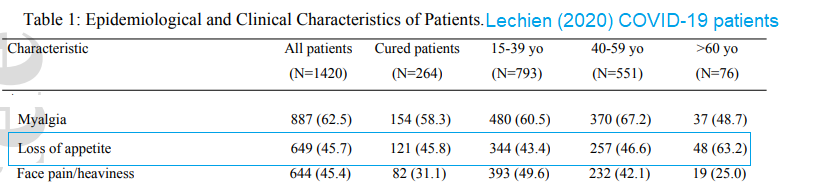
Pain may be defined on multiple levels from the site of injury to the central nervous system. The reader may get a good overview of the many components of pain from this well refereed and referenced Wikipedia article. In this particular study, the operative word is “Myalgia“ translating as pain in one or more muscles.  At the undertaking of this study, myalgia was one of many symptoms of the chronic condition fibromyalgia. The study planners were unable to recruit enough fibromyalgia patients so general neuromuscular pain was allowed as a criterion for acceptance.
Myalgia was found in about 62.5% in all mild to moderate COVID-19 patients (Lechien 2020). These authors published a figure suggesting a link between fever (> 38oC, 45.4%) and myalgia. Interestingly, fatigue was not listed as one of the symptoms in this cohort of over 1000 individuals.
Li and coauthors (2020) examined issue specific, mRNA and protein, public access data bases. The ACE2 enzyme/COVID-19 receptor was found in heart and skeletal muscle. The heart is also a site of injury in COVID-19 infections. Sławiński and Lewicka (2020) discuss Coagulation pathway dysregulation, cytokine storms due to immune system pathway dysregulation, and cardiac troponin T in the blood. The latter suggests direct injury to the cardiac myocytes, perhaps due to expression of ACE2 enzyme/receptor on cardiac myocytes.
Myalgia stories from medical doctors with COVID-19
Dr David Hepburn of the NHS describes COVID-19 muscle pain in this YouTube video describes aching muscles and aching bones. Michael Saag of the University of Alabama describes his describes muscle aches and pain everywhere in his YouTube video.
Going forward
KGK Synergize did a good job of provided unbiased, but only acedoctal suggestions, that Cu(I)NA2  improves myalgia, muscle locking, and fatigue in a very diverse population. How do we go forward with a more defined population who might be experiencing similar symptoms.  Mitosynergy already has anecdotal reports of fever reduction of COVID-19 patients taking Cu(I)NA2. Not everyone in the household who is infected with COVID-19 takes the Cu(I)NA2. While COVID-19 symptoms vary widely, these individuals might be eating similar diets. How might the grip test or the running wheel tests of Takeshita (2018) be adapted to a mild to moderate COVID-19 patient quarantined in his or her home?
- Everyone has some heavy object that can be held with one hand. This object might be a gallon of milk or a suitcase of stored items.
- Many COVID-20 patients report feeling exhausted walking to the bathroom. Patients on the Cu(I)NA2  and skeptical housemates may record distances they may walk about their homes before feeling fatigued.
Ideally data would be collected a day or two before starting the Cu(I)NA2 .
References
Lechien JR, Chiesa-Estomba CM, Place S, Van Laethem Y, Cabaraux P, Mat Q, Huet K, Plzak J, Horoi M, Hans S, Barillari MR, Cammaroto G, Fakhry N, Martiny D, Ayad T, Jouffe L, Hopkins C, Saussez S; COVID-19 Task Force of YO-IFOS.(2020)Clinical and Epidemiological Characteristics of 1,420 European Patients with mild-to-moderate Coronavirus Disease 2019.J Intern Med. 2020 Apr 30. [CrossRef]
Li MY, Li L, Zhang Y, Wang XS.(2020) Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect Dis Poverty. 2020 Apr 28;9(1):45. [PMC free article]
Sławiński G, Lewicka E.(2020)What should a cardiologist know about coronavirus disease 2019? Kardiol Pol. 2020 Apr 24;78(4):278-283. [Cross Ref]
Takeshita H, Yamamoto K, Nozato S, Takeda M, Fukada SI, Inagaki T, Tsuchimochi H, Shirai M, Nozato Y, Fujimoto T, Imaizumi Y, Yokoyama S, Nagasawa M, Hamano G, Hongyo K, Kawai T, Hanasaki-Yamamoto H, Takeda S, Takahashi T, Akasaka H, Itoh N, Takami Y, Takeya Y, Sugimoto K, Nakagami H, Rakugi H. (2018) Angiotensin-converting enzyme 2 deficiency accelerates and angiotensin 1-7 restores age-related muscle weakness in mice. J Cachexia Sarcopenia Muscle. 2018 Oct;9(5):975-986 [PMC free article]
Leave a Reply