The reports keep coming in. This update is all about muscle autoantibodies. A group out of the UK compared auto-antibodies from 84 Covid-19 patients with 32 individuals who had been in the intensive care unit for other reasons. The Covid-19 group was subdivided into 24 who had mild symptoms that did not require hospitalization, 25 with severe Covid-19 whose blood was drawn while in the intensive care, and 35 who had severe Covid-19 whose blood was drawn 3-6 months into recovery. [1] Groups 1-4 were scored via the WHO ordinal Covid-19 severity scale.
1
no
Covid
2
acute
3
severe
6 mo
4
mild
6 mo
pos
tot
%
pos
tot
%
pos
tot
%
pos
tot
%
parietal cell
2
27
7.4
0
25
0
11
36
30.6â€
4
24
16.7
smooth
2
27
7.4
0
25
0
11
36
30.6â€
4
24
16.7
skeletal
1
25
4
4
24
16.7
7
36
19.4**
0
24
0
cardiac
2
21
9.5
1
14
7.1
10
36
27.8***
0
24
0
Table 1 2 ref [1]Only showing tissues for which there are images. All autoantibodies are IgG [1]. ** p = 0.02 (group 2 versus group 3) *** p = 0.005 (group 3 versus group 4). †p = 0.006 (χ2 comparing all groups).
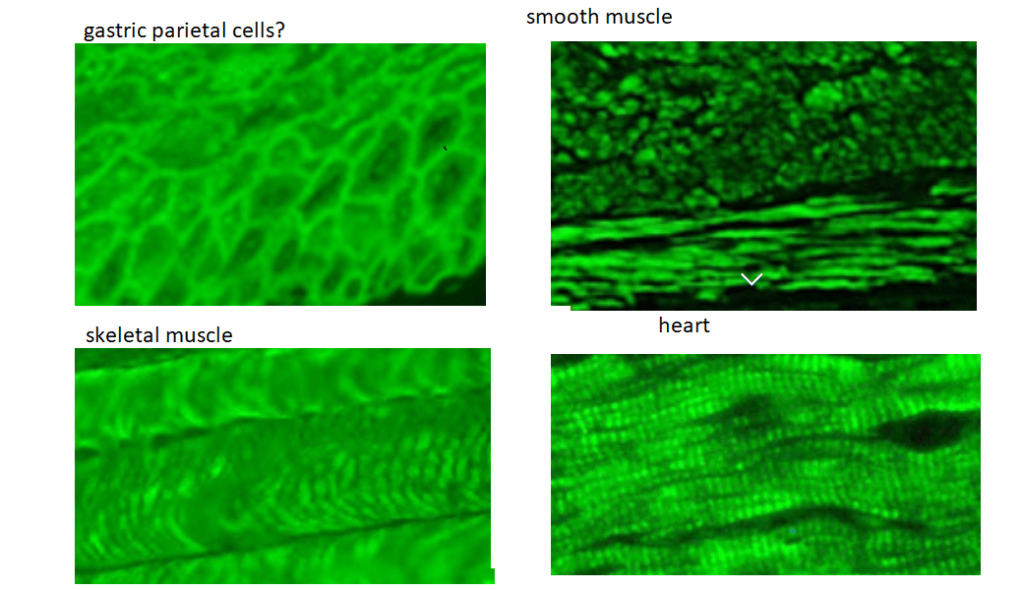
The bottom line is that these antibodies are staining areas that also contain the cytoskeleton protein β-actin.
Figure 1 Some close ups of Figure 2 ref [1]
Rhodamine phalloidin is a dye that binds to this protein called actin. An internet search was performed to find images of gastric parietal cells minus ulcer causing bacteria, heart,
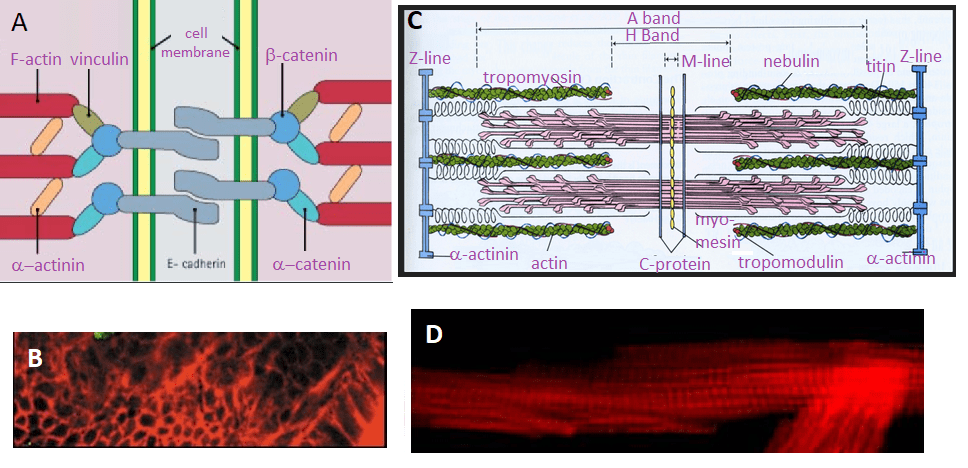
Figure 2 Making sense of Figure 2 of reference [1]. A. Cell adhesion junctions adapted from StudyBlue. B. Actin stainiing of paretal cells. C. The sarcomer from Study Blue. Is valid for both cardiac and skeletal muscle. D. Actom staomomg of cardiac muscle. The red fluorescence corresponds to the A-band.
There is a light area of disagreement with X-axis title in Figure 2 that is a bar graph that lists the percentage of patients in the four groups as a function of the independent variable of 0, 1, 2, and 3 auto antibodies. The heart and parietal cell auto antibody staining looks very much like actin staining with rhodamine phalloidin. Actin and α-actinin are proteins common to parietal cells and the three types of muscle. An autoantigen against α-actinin released from airway or GI tract epithelial cells may cross react with α-actinin isoforms found in smooth, skeletal and cardiac muscle. The Wikipedia actin page list the six isoforms of mammalian actin. This particular Wikipedia page has grown quite extensively in its coverage of the many binding partners of actin in multiple tissue types. The “tissue specific” auto antibodies that very much align where we expect to see actin, could be recognizing actin or anything that binds to actin.
A group out of the United Kingdom took a different approach:
They purchased recominant human IgG1 monoclonal antibodies made against Covid-19 spike protein S1 and S2 domains and SARS-CoV-2 nucleoprotein. [2]
They purchased the following purified proteins: cardiolipin, actin, myelin basic protein (MBP), tropomyosin, ganglioside GM1, insulin, liver microsomes, transglutaminases (tTGs), enolase, beta-amyloid protein, tau protein, somatotropin, human serum albumin (HSA), and dipeptidylpeptidase.
The ability of human and rabbit Covid-19 antibodies to react with their assortment of purified proteins was tested. They used optical density (OD) using an ELISA assay.
Portions of the sequences of Covid-19 proteins were aligned with cytoplasmic actin
Antigens
Spike protein OD
% reactivity
Nucleo protein OD
% reactivity
Envelope protein OD
% reactivity
Membrane protein OD
% reactivity
SARS-CoV-2
3.4
100 ++++
3.76
100 ++++
3.68
100 ++++
3.78
100 ++++
Actin
0.74
17.6 +
1.1
27.1 ++
0.78
18.0 +
0.95
22.2 +
NFP
1.98
56 ++++
0.42
8.5 +
0.27
3.7 –
2
51.1 +++
Alpha-myosin
0.72
17.0 +
0.89
21.3 +
0.36
6.2 +
0.94
21.2 +
Tropomyosin
0.21
1.2 –
0.25
3.8 –
0.25
3.1 –
0.58
12.1 +
Int epi cells
0.49
9.9 +
0.46
9.6 +
2.13
56.0 ++++
0.95
22.2 +
Table 2 From Table 1 reference [2] OD, optical density; NFP, ; Int epi cells, intestinal epithelial cells
SARS-CoV-2 antigen
SARS-CoV-2 sequence
Mapped start to end
Actin sequence
ID (%)
Chain A, Spike protein
GKIQDSLSST
16–25
GSILASLS-T*
60
Chain A, Spike protein
STEKSNII
85–92
STMKIKII*
63
Chain A, Spike protein
IGAGICAS
697–704
IGGSILAS*
63
Chain A, Spike protein
PS–GRLVPR
1,210–1,217
PSIVGR–P
60
Chain A, Nucleoprotein
SSSTKKS
15–21
SSSLEKS
71
Chain A, Nucleoprotein
TEGALNTPK
90–98
TEAPLN-PK
67
Chain A, Spike protein
SVLYNSASFSTF
33–44
SIL—ASLSTF**
58
Chain B, Spike protein
SVLYNSASFSTF
48–59
SIL—ASLSTF**
58
Chain C, Spike protein
SVLYNSASFSTF
48–59
SIL—ASLSTF**
58
Chain E, Spike protein
SVLYNSASFSTF
37–48
SIL—ASLSTF**
58
Chain E, Spike receptor binding domain
SVLYNSASFSTF
48–59
SIL—ASLSTF**
58
FTable 3i From reference [2] regions of Covid-19/SAR-Cov2 that share homology with human β actin.
The human cytoplasmic β-actin as protein blasted against the human database. β-actin shares 94-99% sequence homology to the other five isoforms of mammalian actin.
Figure 3 Blastp results from www.ncbi.nlm.nh.gov/protein
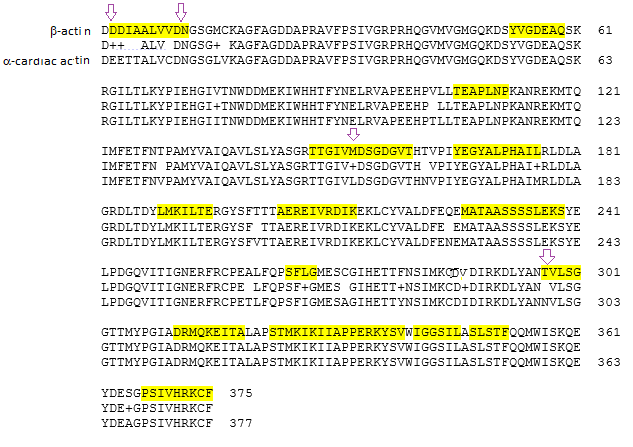
Since we have been examining cardiac tissue in Figure 1 and 2, Figure 3 shows the alignment between and cardiac actin. The top line is the sequence of β-actin, the third cardiac actin, and the middle the sequence homology. A “+” indicates substitution with a similar amino acid . Regions that share homology with Covid protein are highlighted. Note that these overlapping regions also share homology with cardiac actin. Table 5 from reference [2] contains some homology between non spike proteins and β-actin. These include some non structural proteins and helicases.
Figure 4 Alignment of β-actin and cardiac actin with sequences homologous to all the Covid-19 proteins discussed in reference [2]
Coivd-19 patient sera certainly seem to have antibodies that bind to actin in a variety of tissue sections. [1] This report stopped short of showing that these polyclonal antibodies actually recognized actin. [1] Another report demonstrated binding of human recombinant monoclonal antibodies can recognize purified actin. [2] This report offered some nice speculations as to molecular mimicry with the spike protein and other Covid proteins. The implication of the latter report are interesting in that they suggest the potential for developing a Long Covid auto immune disorder from the vaccine. Finally, autoantibodies against an extremely abunant protein like actin imply a major immune response to even a slight injury that releases actin into the circulation. The high degree of homology between actin isoforms of actin only more problematic.
References
Richter AG, Shields AM, Karim A, Birch D, Faustini SE, Steadman L, Ward K, Plant T, Reynolds G, Veenith T, Cunningham AF, Drayson MT, Wraith DC. Establishing the prevalence of common tissue-specific autoantibodies following severe acute respiratory syndrome coronavirus 2 infection. Clin Exp Immunol. 2021 Jun 3. free article
Vojdani, A., Vojdani, E., & Kharrazian, D. (2021). Reaction of Human Monoclonal Antibodies to SARS-CoV-2 Proteins With Tissue Antigens: Implications for Autoimmune Diseases. Frontiers in immunology, 11, 617089. PMC free article
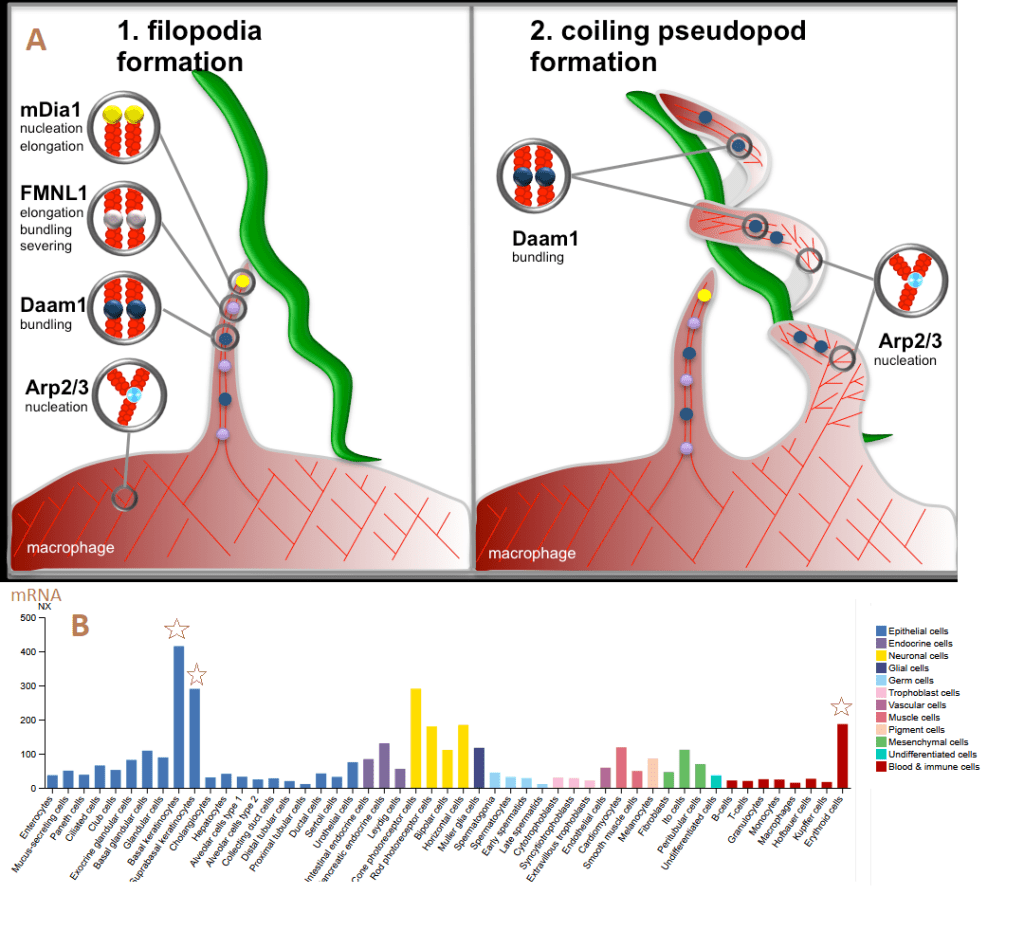
While the world is focused on active and Long Covid, Post Treatment Lyme Disease has many overlapping symptoms. These symptoms have been discussed in the Long Haul Covid post. We have heard plenty about the Covid-19 spike protein and the ACE2 receptor. Borrelia burgdorferi, the bacterium that causes Lyme Disease is a bit more complicated. Figure 1A was taken from the Linder Lab website.
Figure 1. The Daam1 cytoskeletal protein plays a role in internalization of Borrelia A From the Linder Lab website. B. Daam1 mRNA expression in a variety of cell types from ProteinAtlas. RNA single cell type specificity: Cell type enhanced (Basal keratinocytes)
Some of the cell types that express Daam1 (Dishevelled associated activator of morphogenesis 1) might come into our discussion of PTLD and its similarities to Long Covid. The Gilmore Laboratory of the CDC in Fort Collins, CO, USA found that B burgdorferi surface lipoprotein, BBA66, bound the FH2 subunit domain of Daam1. [1] These authors used two neuroglioma cell lines H4 and HS683. [1] To summarize, BBA66 appears to be the equivalent of the Covid-19 spike protein and Damm1 the equivalent of the ACE2 receptor.
Post Treatment Lyme Disease vs Long Covid
It has been suggested that Long Covid will join the ranks of PTLD, myalgic encephalomyelitis /chronic fatigue syndrome, and fibromyalgia post infection syndromes. [5]
Of all of these reported symptoms of PTLD, which ones are best for differentiating recovered patients from those that remain sick form Borrelia or some non related condition? A very large group used a Logistic Regression model and a Decision Tree model. [6] The model development group consisted of 14 recovered and 15 individuals with PTLD symptoms. [6] The validation group included consisted of 13 recovered and 10 with PTLD symptoms. [6] The authors used many different functional questionnaires. They narrowed them down to Three: Neuro-QoL Fatigue t-score (QoLFatigue), the
Wikipedia gives a better explanation of the logit function of the probability of having PTLD based on independent variables of three test scores. This is basically an equation of a straight line in four dimensional space. The authors also discussed correlation of individual PTLD symptoms with one another. Sleep disturbance, fatigue, pain and cognitive complaints were found to interrelate. [6] Given the role of the locus ceruleus and the copper cofactor dopamine beta hydrolase in the sleep-wake cycle. Sleep quality was reported as prominent symptom one year after the active infection in PTLD. [7]
Table 1 comparison of PTLD and Long Covid (LC) symptoms
It has been suggested that Long Covid will join the ranks of PTLD, myalgic encephalomyelitis /chronic fatigue syndrome, and fibromyalgia post infection syndromes. [5]
Of all of these reported symptoms of PTLD, which ones are best for differentiating recovered patients from those that remain sick form Borrelia or some non related condition? A very large group used a Logistic Regression model and a Decision Tree model. [6] The model development group consisted of 14 recovered and 15 individuals with PTLD symptoms. [6] The validation group included consisted of 13 recovered and 10 with PTLD symptoms. [6] The authors used many different functional questionnaires. They narrowed them down to Three: Neuro-QoL Fatigue t-score (QoLFatigue), the
Wikipedia gives a better explanation of the logit function of the probability of having PTLD based on independent variables of three test scores. This is basically an equation of a straight line in four dimensional space. The authors also discussed correlation of individual PTLD symptoms with one another. Sleep disturbance, fatigue, pain and cognitive complaints were found to interrelate. [6] Given the role of the locus ceruleus and the copper cofactor dopamine beta hydrolase in the sleep-wake cycle. Sleep quality was reported as prominent symptom one year after the active infection in PTLD. [7]
Is PTLD a disease of oxidative stress?
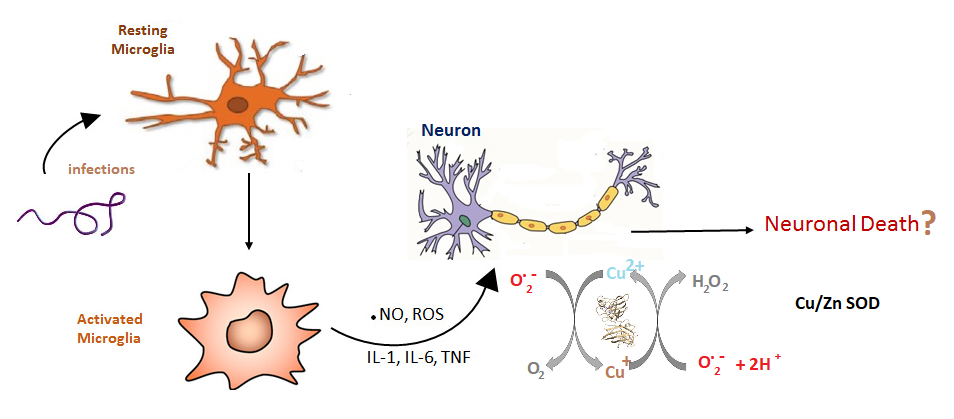
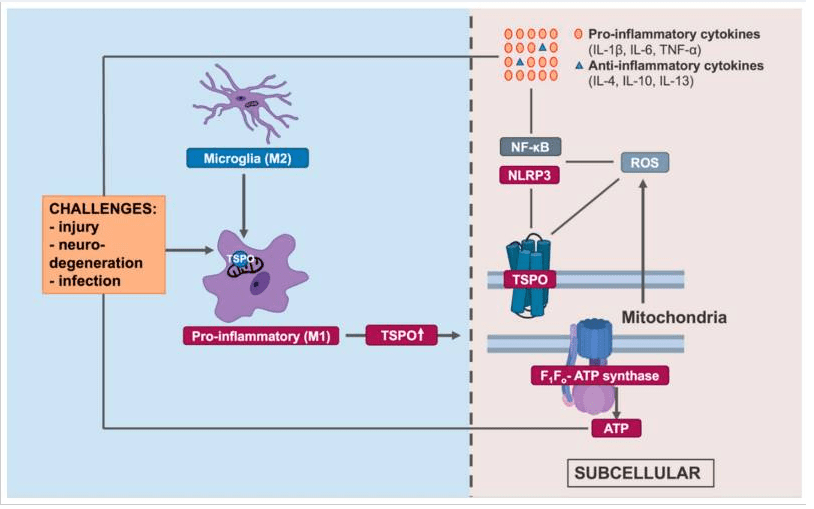
A large group form John Hopkins University School of Medicine used the translocator protein ( TSPO) substrate [11C]DPA-713 to image the brains of patients with PTLD. The translocator protein TSPO is a mitochondrial membrane protein that transports Cholesterol and porphyrins and heme (By similarity) into the mitochondria. [8] A recent review [9] on the influence of TSPO activation and supression on ATP production and subsequent generation of ATP suggests heme transport to the electron transport chain. The expression of TSPO was considered a marker of activated microglia. Activated microglia are phagocytic, cytokine secreted, and antigen presenting immune cells.
Figure 2 from reference [9]. The presence of TSPO suggests activated microglia and some trauma that resulted in their activation.
In the brains of PTLD patients [11C]DPA-713 binding to its target TSPO was increased in the cerebellum, frontal cortex, parietal cortex, thalamus, temporal cortex, and cingulate cortex after controlling for age, BMI, and TSPO genotype. [8]
What this may mean for CopperOne
We don’t know for sure. We don’t know the relative contributions of super oxide and whether a little extra copper would mitigate damage that result for microglia activation. PET imaging with [11C]DPA-713 has become a popular tool for many neuro inflammatory diseases. The PET images only capture one aspect of reactive microglia. Surely the questionnaires, blood cytokines, and serum SOD activity could fill in some gaps.
References
Williams, S. K., Weiner, Z. P., & Gilmore, R. D. (2018). Human neuroglial cells internalize Borrelia burgdorferi by coiling phagocytosis mediated by Daam1. PloS one, 13(5), e0197413. PMC free article
Rebman, A. W., & Aucott, J. N. (2020). Post-treatment Lyme Disease as a Model for Persistent Symptoms in Lyme Disease. Frontiers in medicine, 7, 57. PMC free article
Davis HE, Assaf GS, McCorkell L, Wei H, Low RJ, Reeme Y, Redfield S, Austin JP, Akrami A.Characterizing Long COVID in an International Cohort: 7 Months of Symptoms and Their Impact Cross Ref
Aucott, J. N., & Rebman, A. W. (2021). Long-haul COVID: heed the lessons from other infection-triggered illnesses. Lancet (London, England), 397(10278), 967–968. PMC free article
Turk, S. P., Lumbard, K., Liepshutz, K., Williams, C., Hu, L., Dardick, K., Wormser, G. P., Norville, J., Scavarda, C., McKenna, D., Follmann, D., & Marques, A. (2019). Post-treatment Lyme disease symptoms score: Developing a new tool for research. PloS one, 14(11), e0225012. PMC free article
Weinstein ER, Rebman AW, Aucott JN, Johnson-Greene D, Bechtold KT. (2018) Sleep quality in well-defined Lyme disease: a clinical cohort study in Maryland. Sleep. 2018 May 1;41(5)
Williams, S. K., Weiner, Z. P., & Gilmore, R. D. (2018). Human neuroglial cells internalize Borrelia burgdorferi by coiling phagocytosis mediated by Daam1. PloS one, 13(5), e0197413. PMC free article
Rebman, A. W., & Aucott, J. N. (2020). Post-treatment Lyme Disease as a Model for Persistent Symptoms in Lyme Disease. Frontiers in medicine, 7, 57. PMC free article
Davis HE, Assaf GS, McCorkell L, Wei H, Low RJ, Reeme Y, Redfield S, Austin JP, Akrami A.Characterizing Long COVID in an International Cohort: 7 Months of Symptoms and Their Impact Cross Ref
Turk, S. P., Lumbard, K., Liepshutz, K., Williams, C., Hu, L., Dardick, K., Wormser, G. P., Norville, J., Scavarda, C., McKenna, D., Follmann, D., & Marques, A. (2019). Post-treatment Lyme disease symptoms score: Developing a new tool for research. PloS one, 14(11), e0225012. PMC free article
Aucott, J. N., & Rebman, A. W. (2021). Long-haul COVID: heed the lessons from other infection-triggered illnesses. Lancet (London, England), 397(10278), 967–968. PMC free article
Weinstein ER, Rebman AW, Aucott JN, Johnson-Greene D, Bechtold KT. (2018) Sleep quality in well-defined Lyme disease: a clinical cohort study in Maryland. Sleep. 2018 May 1;41(5)
Coughlin, J. M., Yang, T., Rebman, A. W., Bechtold, K. T., Du, Y., Mathews, W. B., Lesniak, W. G., Mihm, E. A., Frey, S. M., Marshall, E. S., Rosenthal, H. B., Reekie, T. A., Kassiou, M., Dannals, R. F., Soloski, M. J., Aucott, J. N., & Pomper, M. G. (2018). Imaging glial activation in patients with post-treatment Lyme disease symptoms: a pilot study using [11C]DPA-713 PET. Journal of neuroinflammation, 15(1), 346. PMC free article
Betlazar, C., Middleton, R. J., Banati, R., & Liu, G. J. (2020). The Translocator Protein (TSPO) in Mitochondrial Bioenergetics and Immune Processes. Cells, 9(2), 512. PMC free article
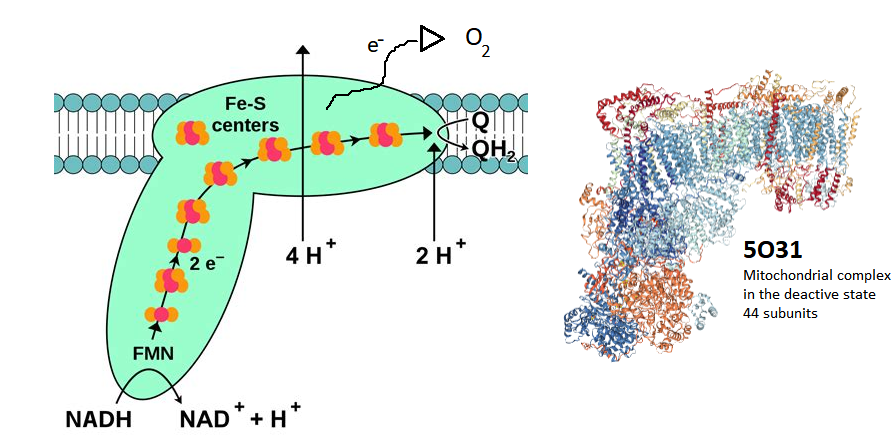
Browsing a January 2021 review on endothelial dysfunction and a potential role of chronic oxidative stress [1] that echoed much of what we’ve had to say about Cu/Zn turning on and off inflammasomes that produce IL1β. They discussed loss of Covid-19 receptor ACE2,more angiotensin II and more super oxide by way of NADPH oxidase. We addressed SOD3 vs the renin angiotensin system in a a slightly different context. These authors led us to ways of looking at Covid-19 proteins. They cited references of papers demonstrating interactions between Covid-19 proteins ORF9c and NSP7 and mitochondrial complex 1 protein NDUFB9 and assembling assisting proteins NDUFAF 1 & 2 that are proposed to be a source of oxygen radicals. [1].
Complex 1 contains at lest 44 protein subunits, one of which is the protein product of the NDUFB9 gene. This gene product is also known as NADH dehydrogenase [ubiquinone] 1 alpha subcomplex subunit 3, the 38 of 46 units. Electrons start at the bottom of the complex and migrate their way to the end to reduce Coenzyme Q. If Covid protein is binding to this complex1 protein, could electrons be diversted to O2?
Some of this is very speculative. If Covid-19 proteins ORF9c and NSP7 bind to Complex 1 proteins in the cell, do they prevent the assembly of complex 1, divert electrons to O2, or nothing at all? Follow this link to learn more about Complex1. Let’s take a look at the molecular fishing expedition.
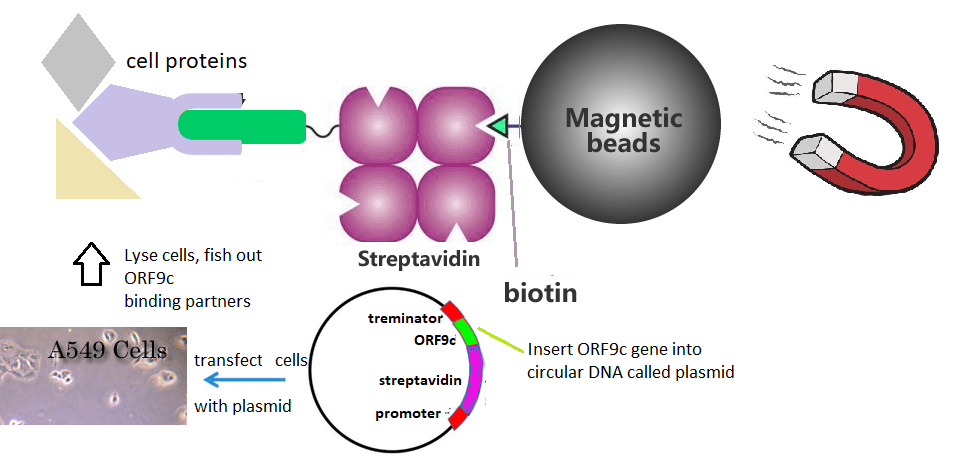
The fishing expedition explained…
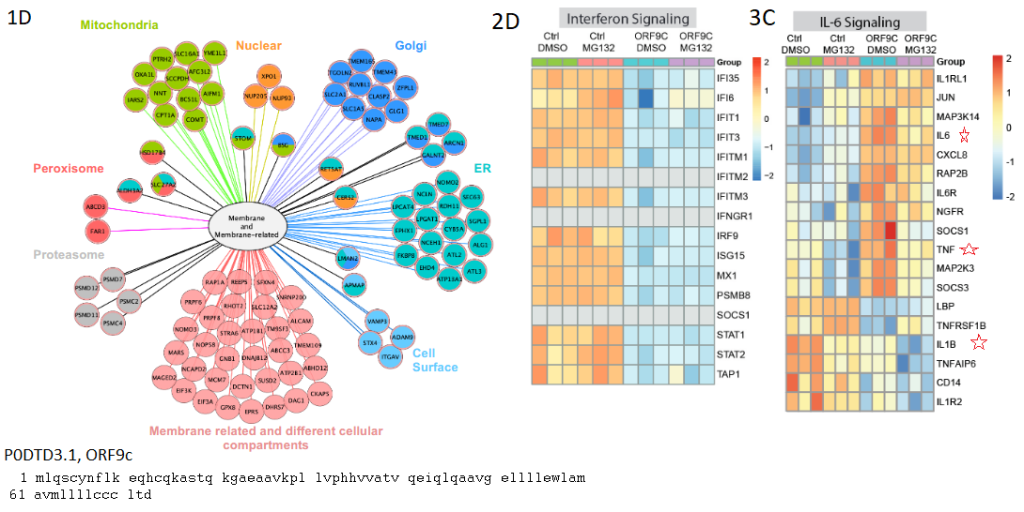
The ORF9c protein with an N-terminal biotin tag was expressed in A549 lung cancer epithelial cells. [1] Streptavidin has a very high affinity for biotin. was used to fish out the ORF9c and what ever mammalian proteins might be binding to it. The authors found that ORF9c binds to many membrane proteins in multiple cell organelles. [2] These authors also found that ORF9c decreased stress and immune related transcripts. [2]. It may be too soon to say if Long Covid is a low grade chronic infection.
The search for binding partners of the protein product of the Covid-19 ORF9c gene in extremely simple terms…
Dominguez and coworkers quickly discovered that the ORF9c gene product associated with proteins in membranes of sub cellular organelles [2]. The authors addressed homology with other membrane associated proteins [2]. They also addressed how expressing this Covid-19 protein in lung epithelial cells, with or without the proeosome inhibitor MG132, affected gene transcription as well as proteins. [2] MG132 was used to inhibit protein degradation via the unfolded protein response. Below are some exerts from a very detailed paper that came to the conclusion that the protein product of the ORF9c gene may help Covid-19 evade the immune system. [2]
Netting cytokine and immune system evasion fish
1D membrane proteins found associated with the ORF9c/svidin chimera from Fig 1D of ref [2] 2D Translated proteins that increased or decreased in abundance. 3C chages in mRNA transcript in IL6 pathways. [2]
Note that the control was a chimera of avidin and a small protein called green fluorescent protein. This serves as a nice control for epithelial cells responding to the translation of unnatural proteins. Changes in protein levels may be due to changes in the translation of mRNAs or to changes in degradation, hence the proteosome inhibitor MG132. STAT1 and STAT2 are are transcription factors that control the expression of interleukins among other proteins. The interferon reducible (IGI) family of proteins will not be addressed in this post. They are involved in Note the increase of cytokine transcripts as well as their receptors in GFP-avidin transfected cells versus ORF9c-avidin transfected cells. Note that the TAP1 protein is down regulated with or without proteosome inhibition. The Herpes virus evades the immune system by blocking the TAP1 protein from transporting viral peptides to the cell surface to alert circulating T cells. Down regulating this protein may have the same effect as blocking it.
References
Chang, R., Mamun, A., Dominic, A., & Le, N. T. (2021). SARS-CoV-2 Mediated Endothelial Dysfunction: The Potential Role of Chronic Oxidative Stress. Frontiers in physiology, 11, 605908. Link
Dominguez Andres, A., Feng, Y., Campos, A. R., Yin, J., Yang, C. C., James, B., Murad, R., Kim, H., Deshpande, A. J., Gordon, D. E., Krogan, N., Pippa, R., & Ronai, Z. A. (2020). SARS-CoV-2 ORF9c Is a Membrane-Associated Protein that Suppresses Antiviral Responses in Cells. bioRxiv : the preprint server for biology, 2020.08.18.256776. Cross Ref
Encephalitis is the inflammation of the brain usually brought on by a viral infection. The N-methyl-D-aspartate receptor is an ion channel for Na+ and Ca2+ that is gated by the synthetic ligand NMDA. Its natural ligands are glycine/D-serine and glutamate. Influx of Na+ and Ca2+ into the cell causes the neuron to depolarize sending an action potential down its axon that results in the release neurotransmitter into the synapse in the vicinity of the dendrites of the post synaptic neuron. Opening and closing of the pore that allows the passage of Na+ and Ca2+ into the cell is gated by the binding of glutamate (Glu) and glycine.
Figure 1 The NMDA receptor A. The NMDA receptor consists of two subunits: NR1 and NR2. Auto antibodies are against NR1 The 5 potential glycosylations were not in the original reference. B. Domains of the NR1 receptor form UniProt.org. C. The typical IgG auto antibody is anticipated to be 50% larger than the NR1 subunit of the NMDA receptor
The authors of a recent review on NMDA receptor encephalitis discuss the correlation of the symptoms with the Ab titers in the CSF rather than the serum. [1]. Teratomas contain multiple cell types and may arise from the ovary or testicle.
A tumor may express the neuronal ion channel. Ovarian teratomas were given as an example. [1]
Herpes simplex virus infections were given as another example. [1] The authors did not speculate as to whether or not a virus must infect neurons in order to trigger production of auto antibodies against neuronal surface proteins.
Unlike the example of the streptococcal M protein resembling cardiac myosin components in rheumatic heart disease, we don’t have an example of compoents of any viral protein resembling the NR1 subunit of the NMDA receptor.
Genetic susceptibility was mentioned as a cause. [1]
Auto antibody binding to the NMDA receptor was mentioned as resembling pharmacology. [1] Which pharmaceuticals? Let’s look at NMDA receptor antagonists. We have the competitive inhibitor Aspartame, the artificial sweetener with neurological side effects. Gabapentin, the anti-convulsant, is a noncompetitive inhibitor. Among NMDA receptor agonists we have the allosteric modulator cholesterol and the partial agonist NMDA.
A journey of the imagination
Just looking at the cartoon in Figure 1A we see that extracellular domain S2 has six potenital glycosylation sites that may offer steric protection from auto antibody binding. Antibodies against the N-terminal domain (NTD) could conceivably block access of glycine. .. or mimic the binding of glycine. Receptor cross linking with a single IgG, what would be the consequences? Some might say receptor endocytosis. The physician treating a patient with unexplained symptoms might order an auto antibody panel to test the CSF. Many of these amateurish questions have been asked in a more sophisticated manner by Dr. Yue-Qiao Huang of Philadelphia College of Osteopathic Medicine Georgia School of Pharmacy and coauthors and coauthors. [2] This review is truly comprehensive and covers many animal models. [2] How do these auto antibodies get past the blood brain barrier in the first place?
Getting auto antibodies past the blood brain barrier
The Wandinger review briefly mentioned a small study that partially answered this question. [1] This study looked for antibody producing plasma cells in the brains of deceased patients who had auto immune encephalitis [3] Some physicians will learn that the blood brain barrier is far more complicated than they may have been taught in medical school. The two main findings of this study were
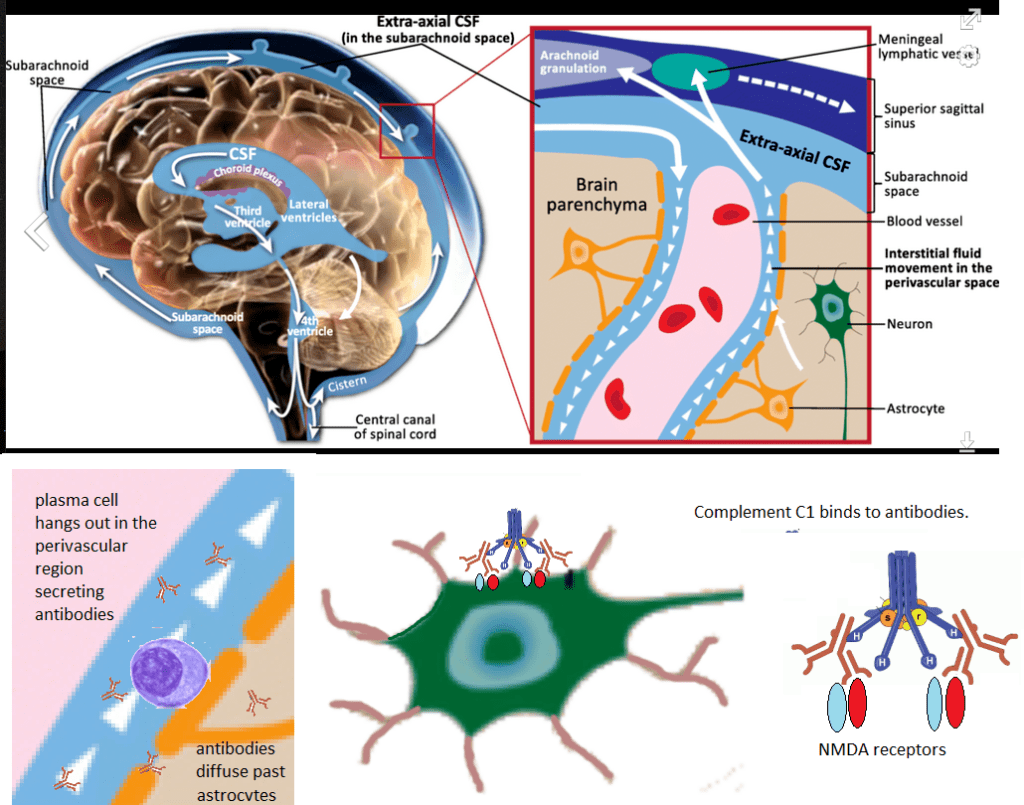
Syndecan / CD138+ cells were found in the brains of diseased patients with anti-NMDAR encephalitis. Syndecan is an extracellular membrane attached protein that was used as a marker for antibody producing plasma cells.[3]. While syndecan may be expressed in multiple organs and cell types, its immuno reactivity was was not found in control brains in this study. [3] These authors reported syndecan staining cells in Virchow-Robin spaces. [3]
These authors also reported complement staining in the brains of of diseased patients with anti-NMDAR encephalitis. [3].
Figure 2, Interpretation of reference [2]. The perivascular space image is from Wikipedia. Antibody secreting plasma cells were shown to hang out in this space, presumably attached to walls using syndecan/CD138. Secreted antibodies can presumably diffuse past the astrocyte barrier to bind to the NR1 subunits of NMDA receptors on neurons. Complement binding was detected in this region.C1 is fllowed by C2-4 and eventually the membrane attack complex C5-9.
Does auto antibody binding to the NMDA receptor mimic pharmaceuticals and/or initiate a membrane attack complex? Most standard treatments seek to turn off all immune response or counter all antibodies, auto or against foreign antigens. Is there a diet that mitigates the migration of plasma cells into this perivascular space?
Case studies
In many of these reports there is a lack of certainty of a causal relationship between a Covid-19 infection and anti-NMDA receptor antibodies. Perhaps the Coivd-19 infection triggered the movement of plasma cells programmed to produce anti-NMDA receptor antibodies into the perivascular spaces of the brain. Did the Covid-19 infection trigger the production of these auto-antibodies?
Case reports of Covid1=9 concombinant with anti-NMDA receptor encephalitis
Management
Management of autoimmune encephalitis is pretty much as we have discussed so far. [10]. This review discusses the pharmacology of antibodies binding to various neurotransmitter receptors that goes beyond what we have discussed so far. [10], Autoimmune-enc ephalitis.org has some interesting things, both positive and negative, about the keto diet. Aside from the ketogenic diet, there really isn’t a diet for autoimmune encephalitis.
References
Wandinger KP, Leypoldt F, Junker R. (2018) Autoantibody-Mediated Encephalitis.Dtsch Arztebl Int. 2018 Nov 5;115(40):666-673. PMC free article
Huang, Y. Q., & Xiong, H. (2021). Anti-NMDA receptor encephalitis: a review of mechanistic studies. International journal of physiology, pathophysiology and pharmacology, 13(1), 1–11. PMC free article
Martinez-Hernandez, E., Horvath, J., Shiloh-Malawsky, Y., Sangha, N., Martinez-Lage, M., & Dalmau, J. (2011). Analysis of complement and plasma cells in the brain of patients with anti-NMDAR encephalitis. Neurology, 77(6), 589–593. PMC free article
Moideen, S., Thomas, R., Suresh Kumar, P. N., Uvais, N. A., & Ul Haq Katshu, M. Z. (2020). Psychosis in a patient with anti-NMDA-receptor antibodies experiencing significant stress related to COVID-19. Brain, behavior, & immunity – health, 7, 100125 PMC free article
Panariello, Adelaide et al. “Anti-NMDA receptor encephalitis in a psychiatric Covid-19 patient: A case report.†Brain, behavior, and immunity vol. 87 (2020): 179-181. PMC free article
Monti, G., Giovannini, G., Marudi, A., Bedin, R., Melegari, A., Simone, A. M., Santangelo, M., Pignatti, A., Bertellini, E., Trenti, T., & Meletti, S. (2020). Anti-NMDA receptor encephalitis presenting as new onset refractory status epilepticus in COVID-19. Seizure, 81, 18–20. PMC free article
Burr, Tyler et al. “N-Methyl-d-Aspartate Receptor Encephalitis Associated With COVID-19 Infection in a Toddler.†Pediatric neurology vol. 114 (2021): 75-76. PMC free article
Sarigecili, E., Arslan, I., Ucar, H. K., & Celik, U. (2021). Pediatric anti-NMDA receptor encephalitis associated with COVID-19. Child’s nervous system : ChNS : official journal of the International Society for Pediatric Neurosurgery, 1–4. Advance online publication. PMC free articles
McHattie, A. W., Coebergh, J., Khan, F., & Morgante, F. (2021). Palilalia as a prominent feature of anti-NMDA receptor encephalitis in a woman with COVID-19. Journal of neurology, 1–3. PMC free article
Macher S (2018) Management of Autoimmune Encephalitis: An Observational Monocentric Study of 38 Patients. Front. Immunol., 22 November 2018 PMC free article
This post reviews a few recent reports in the literature concerning niacin, the other two thirds of CopperOne, and Covid. Most of the latest are nice reviews and novel ideas. Then there is a review that forces us to say, “Wow! CopperOne may modulate our immune response to more infections than Covid-19.
Some very nice reviews,clever in silico, and in lab experiments
Min Su and coauthors (Guangxi Key Laboratory of Tumor Immunology and Microenvironmental Regulation, Guilin, China) published some interesting ideas concerning the gene overlap of treating colorectal cancer (CRC) and Covid-19 with niacin. [1] We’ve covered a lot of similar concepts in niacin benefits infections. These authors suggested that niacin might actually bind to the inflammatory cytokine IL-1β They came to this conclusion using in silico molecular docking techniques. [1]
The angiotensin converting enzyme 2 is not just for proteolysis of angiotensin II. Camargo and coauthors remind us that this protease can also form heterodimers with the broad neutral ammino acid transporter (B0AT). [2] We are also reminded that mutations in B0AT cause Hartnup Disease which has pellegra like symptoms. If Covid-19 abinds to ACE2 receptors in the small intestine brush borders, the absorption of amino acid precursors of niacin and serotonin might be compromised. [2] Niacin supplementation might be required. [2]
Doroftei and coauthors published an extensive review of niacin/NADH on many biological pathways as they pertain to oxidative stress and Covid-19 infections. [3]
Niacin has been shown to bind to the main 3CLpro protease of Covid-19 and modestly inhibit it’s activity. [4]
And this is how CopperOne works!
Or so we like to think..
This review was authored by Melinda Suchard Dana M. Savulescu of National Institute for Communicable Diseases, Johannesburg, South Africa. Dr Suchard is an expert in the role of indoleamine 2,3-dioxygenase (IDO) in infectious diseases. These authors define “sepsis” as the body’s response to an infection. Septicemia is defined as infectious particles in the blood.
Nicotinamide and macrophage phenotypes
The reducing eqquivalent nicotinamide may be derived from dietary niacin, recycled through existing the reduced version, or synthesized de novo from the amino acid tryptophan. The rateâ€limiting enzyme for de novo nicotinamide synthesis is IDO, a haemâ€containing intracellular enzyme found predominantly in cells of the macrophage/monocyte lineage. [5]
M1 macrophages secrete proâ€inflammatory cytokines such as TNF alpha and interleukin 1â€Î².
M2 macrophages secrete cytokines such as interleukinâ€10, which have immune suppressive functions and play a role in wound healing.
Immunometabolism in macrophages
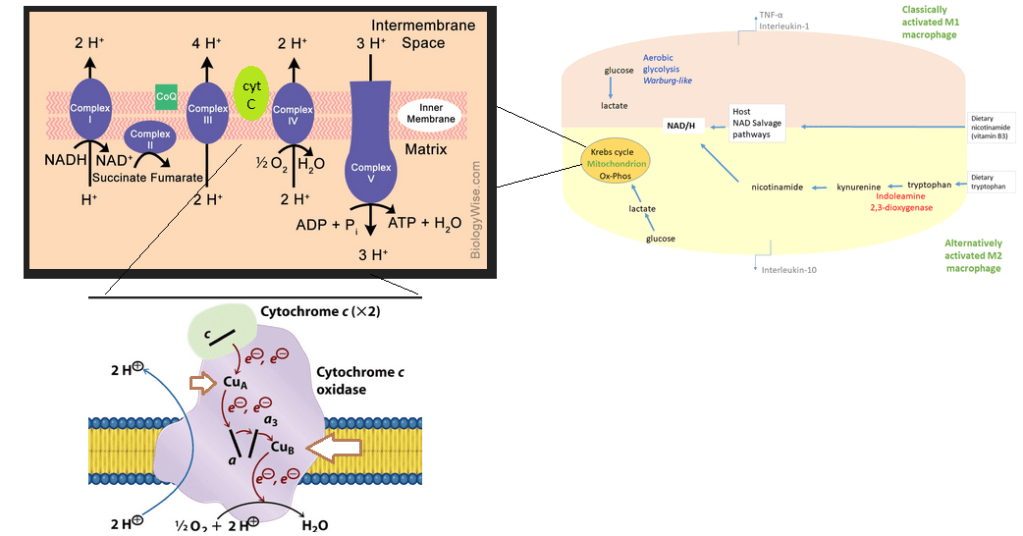
Resting macrophage utilize the TCA cycle to generate NADH that feeds into the electron transport chain to generate ATP. When stimulated with pathogens macrophage switch to glycolysis. This Warburg metabolism is also found in cancer cells. While not as efficient as aerobic respiration, stopping at pyruvate allows the macrophage to conserve pyruvate for synthesis of other biological materials.
Right images of the role of copper in the mitochondria. Left from ref [5]
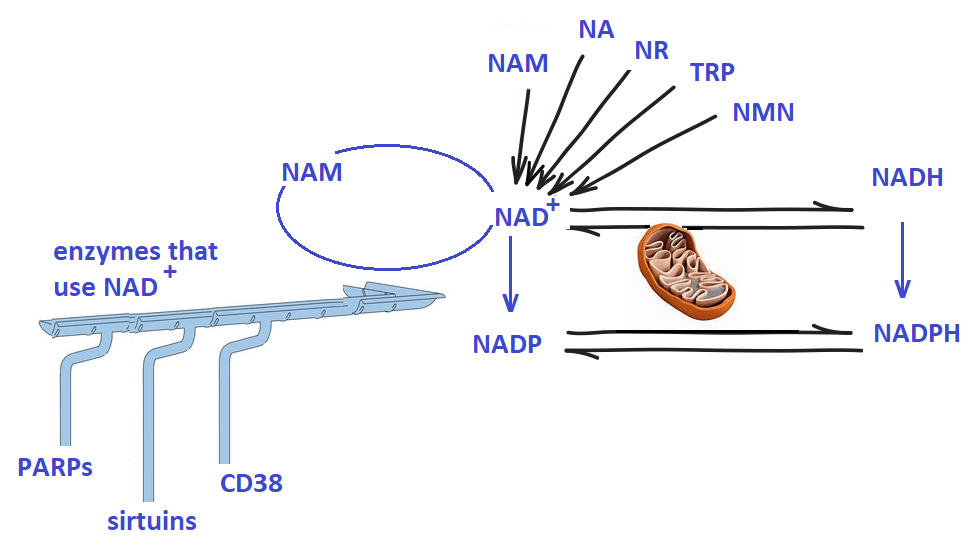
A closer look at pathways intersecting with NAD+
The authors looked at pathways regulated by NAD+, the oxidized form of NADH + H+,. from the standpoint of IDO kicking in, or not, when dietary niacin is insufficient. These pathways include:
PARPADP ribose polymerase enzymes use NAD+ as a substrate to repair DNA double strand breaks.
NAD+ also plays a key role in autophagy through partnering with sirtuins, which are NADâ€dependent deacetylases.
CD38can act as an extracellular receptor for NAD+ and an enzyme that produces ADP ribose from NAD+.
NAD+ is released from cells during early inflammation where it may interact with CD38 on T and B lymphocytes. [5] CD38 may also be found on airway smooth muscle cells. [5]
M1 macrophage activation occurred simultaneously with NAD+ depletion .
Nuclear NAD+ may affect transcription of key inflammatory genes.
Looking forward
The Suchardand Savulescu review on NAD+ pathways in macrophage may change how we view a lot of things beyond Covid and the immune system.
Note the role of both NAD+ and ATPSummary of NAD+ pathways NAM, nicotinamidr; NA, nicotinic acid; NR, nicotinamide riboside; Trp, tryptophan; NMN, Nicotinamide mononucleotide; NAD+, oxidized Nicotinamide adenine dinucleotide; NADH, reduced NAD+; NADP, Nicotinamide adenine dinucleotide phosphate; NADPH, reduced NADP. All NAD+ signalling is very responsive to an active electron transport chain in the mitodhondria. NAD+ may be recycled or siphoned off to other enzymes.
The added component of CD38 signalling, that we are only now becoming aware of, adds a whole new component of how Cu+ and nicotinic acid may act in synergy as an immune modulator agent. And a lot more!
References
Li, R., Li, Y., Liang, X., Yang, L., Su, M., & Lai, K. P. (2021). Network Pharmacology and bioinformatics analyses identify intersection genes of niacin and COVID-19 as potential therapeutic targets. Briefings in bioinformatics, 22(2), 1279–1290. PMC free article
Camargo SMR, Vuille-Dit-Bille RN, Meier CF, Verrey F. (2020) ACE2 and gut amino acid transport. Clin Sci (Lond). 2020 Nov 13;134(21):2823-2833.
Doroftei, B., Ilie, O. D., Cojocariu, R. O., Ciobica, A., Maftei, R., Grab, D., Anton, E., McKenna, J., Dhunna, N., & Simionescu, G. (2020). Minireview Exploring the Biological Cycle of Vitamin B3 and Its Influence on Oxidative Stress: Further Molecular and Clinical Aspects. Molecules (Basel, Switzerland), 25(15), 3323. PMC free article
Gao, J., Zhang, L., Liu, X., Li, F., Ma, R., Zhu, Z., Zhang, J., Wu, J., Shi, Y., Pan, Y., Ge, Y., & Ruan, K. (2020). Repurposing Low-Molecular-Weight Drugs against the Main Protease of Severe Acute Respiratory Syndrome Coronavirus 2. The journal of physical chemistry letters, 11(17), 7267–7272. Free PMC article
Suchard MS, Savulescu DM. Nicotinamide pathways as the root cause of sepsis – an evolutionary perspective on macrophage energetic shifts. FEBS J. 2021 Mar 8. Free article
Part of the challenge of finding a treatment is finding a good diagnosis of the problem. What is the Long Covid problem anyway? Long Covid seems a lot like a continuation of the active infection minus the virus shedding. This post examines some of the basic toxicology outcome measures that may or may not lead us to an understanding and ultimately a treatment.
Cytokine profiles
McFarland and coauthors have made a case for how inflammatory cytokines can lead to nociceptor sensitization in dorsal root ganglia.[1] The dorsal root ganglion, as you may recall, is the nodule containing the cell bodies of afferent neurons of the dorsalroot. Afferent neurons contact somatosensory end organs in the skin, deep tissue and viscera.
the Dx
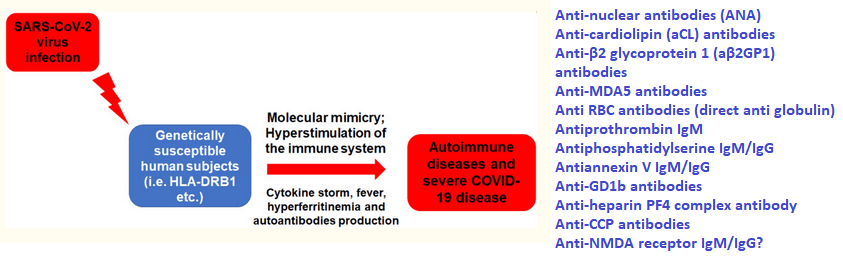
Clinical trials of treatments of active Covid infections have proposed monitoring IL-1β, IL-10, IL-6, IL-18. IL-1β , IL-6, tumor necrosis factor (TNF), and other cytokines were listed as drivers of Long Covid chronic pain. [1] IL-10 is generally considered anti-inflammatory, but has been argued to be pro-inflammatory in Covid-19, cancer, and autoimmune diseases. [2] If the damage is done, what is the point of measuring cytokines as an outcome measure? Long Covid has been proposed to be an autoimmune disease. [3]
Figure 1 adapted from reference [3].
Reference [3] did not mention anti-NMDA receptor antibodies in Covid patients but we have covered thie phenomenon elsewhere on this website. When it comes to chronic pain, it is all about PGE2 that comes after inflammatory cytokines. One question not answered by this review is if auto antibodies binding to their targets sets off a new cytokine storm of diagnostic value.
The Rx
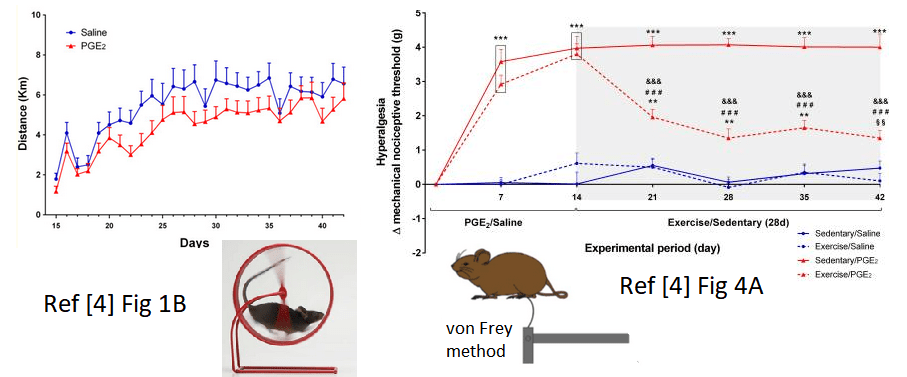
In an animal model mouse pindpaws were intraplantar injected with PGE2 or saline in control for 14 consecutive days [4]. After that mice had free access to running wheels for 28 days or were forced to remain sedentary. [4] During the expercise period mechanical hyperalgesia was measured by the electronic von Frey method.[4]
Figure 1, highlights from ref [4] Figure 1B, how much the mice ran on their wheels during the course of he study Figure 4A analgesia induced by voluntary running Data are showed as mean ± SEM (N = 8–10 per group) (***p≤0.001, different from both sedentary/saline and exercise/saline groups; ###p≤0.001, different from sedentary/PGE2 group; **p≤0.01, different from both sedentary/saline and exercise/saline groups; §§p≤0.01, different from exercise/saline group; &&&p ≤ 0.001, different from the time point 14d of the same group)
The images shown n Figure 2 are only a small sampling of a remarkable study. [4] The authors did not attempt to establish a molecular mechanism of exercise induced analgesia. They discussed anti-inflammatory cytokines and the endocannabinoid system as possibilities. Likewise, we do not know if PGE2 DRG sensitization or NMDA auto antibodies are the cause of hyperalgesia. Whether Long Covid hyperalgesia is the result of PGE2 induced modifications of the DRG or auto antibodies, exercise therapy if human patients can be convinced to walk or run 6 km per day like the mice.
Complete blood counts and more
While Long Covid is hitting the peer reviewed literature, there really hasn’t been the extensive work linking parameters uncovered by the complete blood count to symptoms. One study that we know about has followed CBC parameters up to 21 days after symptom onset. [5] At present we are not aware if neutrophil counts stay high and lymphocyte counts stay low in those with the Long Covid syndrome. One would hope that as new treatments for Long Covid undergo clinical trials, CBC will be part of the toxicology tests of an agent on a new population. A complete blood count and all the associated blood chemistry has been conducted on a 57 year old man who presented with autoimmune hepatitis. [5]
We may be required to obtain complete blood counts when testing Cu(I)NA2 on a new population. If we suspect an autoimmune disease, we may want think about sub typing lymphocytes.
Liver Enzymes
The same study reported liver enzymes in the serum of the 57 year old male Long Covid patient.[6]
parameter
patient
reference range
Alkaline phosphatase
48 U/l, repeat 29 U/l
39–117 U/l
Aspartate aminotransferase
137 U/l, repeat 371 U/l
0–40 U/l
Alanine aminotransferase
106 U/l, repeat 246 U/l
0–44 U/l
GGT
655 U/l
0–65 U/l
Prothrombin time
10.4 seconds
9.1–12 seconds
International Norm. Ratio
1
0.8–1.2
Partial thromboplastin time
28 seconds
24–33 seconds
Total iron binding capacity
271 μg/dl
250–450 μg/dl
Iron
222 μg/dl
38–169 μg/dl
Iron saturation
82%
15–55%
Ferritin
860 ng/ml, repeat 3,275 ng/ml
30–400 ng/ml
Erythrocyte sedimentation rate
66 mm/hr
0–30 mm/hr
Haemoglobin A1c
5.90%
4.8–5.6
Anti-smooth muscle Ab
83 units
Positive >30 units
Anti-mitochondrial Ab
174.5 units
Positive >24.9 units
Anti-double-stranded DNA Ab
14 IU/ml
Positive >9 IU/ml
Anti-soluble liver antigen Ab
4.4 units
Negative 0–20 units
Exerts from Table 1 of reference [5] Antibody, Ab; Gamma-glutamyl transferase, GGT;
The authors concluded that this male had auto immune cirrhosis. [7] Liver enzymes are clearly elevated. It is not really clear if the antibodies against smooth muscle proteins contributed to the cirrhosis or if these antibodies affected other organs. Albumin, produced by the liver, was within the reference rage (not shown). Immunoglobins were elevated. Future studies with Cu(I)NA2 to to treat long Covid should include normal blood work that includes liver enzymes. Indeed studies in humans (5-FU toxicity) and rodents (fatty liver model) have shown that Cu(I)NA2 mitigates liver damage.
Standard blood chemistry may be good enough for diagnosing post Covid liver damage. Post Cu(I)NA2 blood chemistry tests may tell us if we have a treatment.
D-dimer
D-dimer is a degradation product of fibrin, the stuff of blood clots. The presence of D-dimer in the blood is an indication of thrombosis, the formation of a blood clot inside a blood vessel. The first report summarized the clinical assessment of 384 patients reviewed a median of 54 (IQR 47–59) days following hospital discharge with COVID-19. [7] Another study found that Long Covid patients with elevated D-dimer tended to be younger and did not require hospitalization. [8] Did the formation of vascular blood clots prevent deleterious internal bleeding? Was vascular damage in the patients with D-dimers long into recovery also severe enough for vascular smooth muscle proteins to be released into the blood and trigger an auto immune reaction? [6]
Figure 3 The stages of clotting. Smooth muscle proteins may be exposed to antigen presenting cells during the initial injury.
If cirrhosis is brought on by damaged blood vessels in the liver, could copper and other nutrient absorption result from damage to blood vessels in the gut? This relates to copper deficiency and eye health problems being brought on by gastric bypass surgery.
A month after the original posting of this post, there have been no new reports of actin auto antibodies in Long Covid to the best of our knowledge. This is probably not something we want to include as a diagnostic of Long Covid and efficacy of Cu(I)NA2.
Dx
We might ask for information s to whether D-dimer was high during the active covid Infection. This might diagnose that vascular damage probably occurred. We can test serum copper bound to ceruloplasmin or something.
Rx
Lysyl oxidase is needed to cross link collagen in damaged blood vessels.
Post treatment Lyme Disease (PTLD) and Long Covid questionnaires
Our previous experience with the Revised Symptom Impact Questionnaire (SQIR) helped us understand how Cu(I)NA2 might be acting in a population with a diverse set of symptoms of nerve/muscle discomfort. Long Covid and PTLD share overlapping symptoms. Might there be a better or an additional questionnaire for long Covid? A previous study used four questionnaires to assess PTLD
Fatigue Severity Scale (FSS) A nine item fatigue metric has summary scores that range from 9 to 63 with a higher score indicating worse fatigue, and with ≥36 indicating clinically relevant levels of fatigue [10]
Short-Form McGill Pain Questionnaire (SF-MPQ) A 15-item pain metric has summary scores that range from 0 to 45 with a higher score indicating worse pain, and with ≥4 indicating a clinically significant experience of pain [11]
Pittsburgh Sleep Quality Index (PSQI) This test has summary scores ranging from 0 to 21 with a higher score indicating worse sleep quality, and with ≥6 indicating clinically significant poor sleep quality. [12]
The Beck Depression Inventory (BDI) is a 21 item depression questionnaire with summary scores ranging from 0 to 63 with a higher score indicating worse depression, and with ≥14 indicating mild, moderate, or severe depression. [13]
The PTLD study concluded that PTLD patients had a lower quality of life than normal controls. [9] These questionnaires may be useful in evaluating Cu(I)NA2 in the treatment of Long Covid-19 and PTLD. Previous experience has suggested that participants might become impatient with too many questions and not give much thought to the answers. A very old questionnaire from 1977 [14] addresses fatigue, pain, and sleep disturbances. [14] The authors were trying to correlate autonomic nervous system function that included “sweaty palms” and “difficulty breathing” with depression and anxiety. [14] Only 24 questions with scores ranging from “very frequently” to “rare or never” may represent less of a challenge to the participant to thoughtfully answer.
Dx tests to keep or not in active vs Long Covid
Cytokine profiles were all the 2020 rage with active Covid, but may or may not be worth the cost and health risks of dealing with infectious blood samples. ORF9c certainly adds an interesting twist if Covid-19 can evade our immune systems in Long Covid.
If Long Covid is auto immune, CBC is a good and inexpensive test to keep.
If Long Covid is auto immune, liver enzymes are a good and inexpensive test to keep.
D-dimer is sort of iffy. The publication source pointed to anti-smooth muscle auto-antibodies that went along with D-dimer. The developing Covid literature is simply not supporting this one.
Quality of Life Questionnaires. Long Covid and PTLD share overlaps. We could ask direct questions as to CDC’s list of active and long Covid symptoms. There is a short and sweet questionnaire that could be informative in conjunction with direct symptom questions that addresses the hypothesis that Cu(I)NA2 helps autonomic nervous system functions. [13]
References
McFarland AJ, Yousuf MS, Shiers S, Price TJ. (2021) Neurobiology of SARS-CoV-2 interactions with the peripheral nervous system: implications for COVID-19 and pain. Pain Rep. 2021 Jan 7;6(1):e885. Free PMC article.
Lu L, Zhang H, Dauphars DJ, He YW.(2020) A Potential Role of Interleukin 10 in COVID-19 Pathogenesis. Trends Immunol. 2021 Jan;42(1):3-5. doi: 10.1016/j.it.2020.10.012. Epub 2020 Nov 2. PMID: 33214057 Free PMC article. Review.
Halpert G, Shoenfeld Y. (2021) SARS-CoV-2, the autoimmune virus. Autoimmun Rev. 2020 Dec;19(12):102695. Free PMC article.
Sartori, C. R., Pagliusi, M., Jr, Bonet, I., Tambeli, C. H., & Parada, C. A. (2020). Running wheel exercise induces therapeutic and preventive effects on inflammatory stimulus-induced persistent hyperalgesia in mice. PloS one, 15(10), e0240115. https://doi.org/10.1371/journal.pone.0240115 PMC free article
Singh, B., Kaur, P., & Maroules, M. (2021). Autoimmune Hepatitis-Primary Biliary Cholangitis Overlap Syndrome Triggered by COVID-19. European journal of case reports in internal medicine, 8(3), 002264. https://doi.org/10.12890/2021_002264 Free PMC article
Mandal S, Barnett J, Brill SE, Brown JS, Denneny EK, Hare SS, Heightman M, Hillman TE, Jacob J, Jarvis HC, Lipman MCI, Naidu SB, Nair A, Porter JC, Tomlinson GS, Hurst JR; ARC Study Group. ‘Long-COVID’: a cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax. 2020 Nov 10:thoraxjnl-2020-215818. doi: 10.1136/thoraxjnl-2020-215818. Epub ahead of print. PMID: 33172844; PMCID: PMC7661378. Free PMC article
Lanini, S., Montaldo, C., Nicastri, E., Vairo, F., Agrati, C., Petrosillo, N., Scognamiglio, P., Antinori, A., Puro, V., Di Caro, A., De Carli, G., Navarra, A., Agresta, A., Cimaglia, C., Palmieri, F., D’Offizi, G., Marchioni, L., Kobinger, G. P., Maeurer, M., Girardi, E., … Ippolito, G. (2020). COVID-19 disease-Temporal analyses of complete blood count parameters over course of illness, and relationship to patient demographics and management outcomes in survivors and non-survivors: A longitudinal descriptive cohort study. PloS one, 15(12), e0244129. https://doi.org/10.1371/journal.pone.0244129 Free PMC article
Townsend L, Fogarty H, Dyer A, Martin-Loeches I, Bannan C, Nadarajan P, Bergin C, O’Farrelly C, Conlon N, Bourke NM, Ward SE, Byrne M, Ryan K, O’Connell N, O’Sullivan JM, Ni Cheallaigh C, O’Donnell JS. Prolonged elevation of D-dimer levels in convalescent COVID-19 patients is independent of the acute phase response. J Thromb Haemost. 2021 Feb 15. doi: 10.1111/jth.15267. Epub ahead of print. PMID: 33587810. Cross Ref
Rebman AW, Bechtold KT, Yang T, et al. . The clinical, symptom, and quality-of-life characterization of a well-defined group of patients with posttreatment Lyme disease syndrome. Front. Med. 2017;4:224 10.3389/fmed.2017.00224 [PMC free article]
Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. (1989)The Fatigue Severity Scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol46(10):1121–3.10.1001 [CrossRef]
Melzack R. (1987)The short-form McGill Pain Questionnaire. Pain 30(2):191–7.10.1016/0304-3959(87)91074-8 [CrossRef]
Buysse DJ, Reynolds CF, III, Monk TH, Berman SR, Kupfer DJ. (1989) The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 28(2):193–213.10.1016/0165-1781(89)90047-4 [CrossRef]
Beck A, Steer R, Brown G. (1996) Beck Depression Inventory – Second Edition Manual. San Antonio: The Psychological Corporation; . [Google Scholar]
Neziroglul F, Yaryura-Tobias JA (1977) Development of an Autonomic Nervous System Questionnaire: Diagnostic Aid in Measurement of Anxiety, Depression, and Aggression. ORTHOMOLECULAR PSYCHIATRY, VOLUME 6, NUMBER 3, 1977, Pp. 265-271 [free article]
This post has been updated 04 May 2021. Quoted from the blogpage of NIH director Francis Collins, “If you’d like to find a way to pitch in and help, getting involved in the COVID Symptom Study is as easy as downloading the app.”
How do the symptoms of the active Coivd-19 infection compare with “Long Haul” Covid symptoms that linger after the infection has cleared?
Active Covid-19 versus long haul
Covid-19 active infection [1]
Long haul Covid-19 symptoms [2]
comments
fatigue
fatigue
Shortness of breath or difficulty breathing
Shortness of breath
cough
Cough
Muscle or body aches
Muscle pain
Chest pain
noticeable in active infection?
Joint pain
Rheumatoid arthritis?
Head ache
Head ache
Heart palpitations
Depression
Brain fog
Fever or chills
Intermittent fever
New loss of taste or smell
Smell/taste loss
less common in long haul
Sore throat
Congestion or runny nose
Nausea or vomiting, diarrhea
Comparison of CDC symptoms of active Coivd-19 and long term Covid-19
The gastrointestinal symptoms seem to be restricted to the active infection. Neurological symptoms seem to be features of long haul Covid-19.
According to the CDC less common symptoms may also include cardiac inflammation, renal injury, rashes, and hair loss. Skin rashes and hair loss may also be part of the less common long term symptoms of Covid-19. [2]
Covid-19 and rheumatoid arthritis cytokines
A report from June of 2020 points out that many of the cytokines observed in active Coivd-19 infections are also observed in Rheumatoid arthritis, an autoimmune disorder affecting the joints.[3] According to these authors back in June of 2020, a small percentage of Covid-19 patients experience arthalgia. [3]
Exhausted T cells and neurological symptoms of Covid-19
A report from January of 2021 correlated neurological symptoms of Covid-19 with dediffferentiated monocytes and “exhausted” T cells in the cerebral spinal fluid (CSF). [4]. Neurological Covid-19 symptoms may include anosmia, ageusia, headache, dizziness. Some of the causes may include damage from oxygen deprivation, hyperpyrexia, direct viral damage, or indirect damage from immune sytem activation [4]. Exhausted T cells were defined by cell surface receptors. [4] T cell exhaustion can also be described as a metabolic phenomenon that occurs when T cells migrate into a nutrient poor environment. [5] The mitochondrial transcription factor Peroxisome proliferator-activated receptor gamma co-activator 1-alpha (PGC-1α) is given able discussion in this review of the role of mitochondria in the life cycle of T cells. [5] It may be worth noting that body temperature and heart rate are under brain stem control.
The role of the gastrointestinal tract
Note that gastrointestinal symptoms are largely ignored in long haul Coivd-19 Zhang and co authors used resources at proteinatlas.org to make a argument that the gastrointestinal symptoms seen in Covid-19 could be explained by the presence of angiotensin converting enzyme 2 (ACE2) receptor for Covid-19 being expressed on the these cells [6]. The need for copper supplements to preserve eye health in a Cu for gastric bypass patients post. Part of the stomach and duodenum are removed in this operation. Much of our dietary copper is absorbed in this same region.
From proteinatlas.org Expression of the Cu+ absorbing channel Ctr1 and the Covid-19 receptor ACE2.
Note that both the duodenum and rest of the small intestine express medium levels of Ctr1 with smaller levels of expression in the stomach and colon. Note that the duodenum and small intestine express more ACE2 than the bronchus and nasopharynx. We can certainly make the argument that in ab active Covid-19 infection with diarrhea, the stomach absorption of Cu+ may be the only option.
An international survey of 3762 “Long Covid” patients
revealed several trends [7]:
“Brain fog” or some form of cognitive impairment occurred in 85.1% (3203). For instance, over 80% were mildly or seriously unable to make serious decisions or work. [7]
Memory impairments were reported in 72.8% of the respondents. Only 20% were mildly or seriously unable to return home without getting lost. Remembering medication was experienced by 60% of the respondents.[7]
Difficulties with speech and language was experienced by about half of the respondents. These difficulties included word retrieval, communicating verbally, and processing written text. [7]
Sensorimotor symptoms were experienced by about 80% of the respondents. These symptoms included pins and needles, electric zaps, coldness in a body part, facial numbness, and more. [7]
Sleep disturbances were experienced by about 80%. These disturbances ranged from insomnia and restless legs to changes in dreams. About a fifth of those that experienced these symptoms had similar issues prior to Covid-19.
Headaches were reported in 77% of the respondents. [7]
Emotion and mood disturbances were reported by about 8% of the respondents. These disturbances ranged from apathy, difficulty controlling emotions, irritability, anxiety, and depression. Over half that reported post Covid anxiety and depression did not have these symptoms prior to Covid.[7]
Lost of taste and/or smell was experienced by about 60% of the respondents. About a third experienced lost of taste and another third experienced a lost of smell leading the reader to conclude that the phenomenon tended to be “either or.” Respondents also reported phantom smells that tended to be smoke and cigarettes. [7]
Hallucinations were primarily olfactory (25%) with 10% or less experiencing visual, auditory, or tactile hallucinations. [7]
Fatigue or post exertion al malaise were experienced by close to 80%.
Low and high grade fevers were also common. [7]
Is Long Covid many syndromes?
One study [8] suggests long Covid is actually four syndromes:
permanent damage to lung and heart A recent in the journal Nature suggests that Long Covid may be an autoimmune disease. [9] Auto-antibodies against the annexin A2 are important as because annexin A2 helps maintain membrane in small blood vessels of the lung.[9] Streptococcus pyrogens M protein mimics proteins in the heart explaining how strept throat can lead to rheumatic fever. [9]
post-intensive care syndrome has been hypothesized to be due to a breakdown of the hypothalamic-pituitary-adrenal (HPA) axis and related to chronic fatigue syndrome. [10] The author proposed that the cytokine IL-1β, that is a hallmark of Covid-19 infections, is known to modulate CRH release by the hypothalamus. It was proposed that related series of events lead to adrenal atrophy.
post-viral fatigue syndrome, also myalgic encephalomyelitis/chronic fatigue syndrome It has been argued that CFS has at its roots mitochondrial coenzyme Q10 deficiency and that CoQ10 supplementation may help Long Covid sufferers. [11] Oxidative stress associated with mitochondrial dysfunction was also reviewed.
long term covid symptoms It is not clear what the authors meant by this 4th explanation of Long Covid.
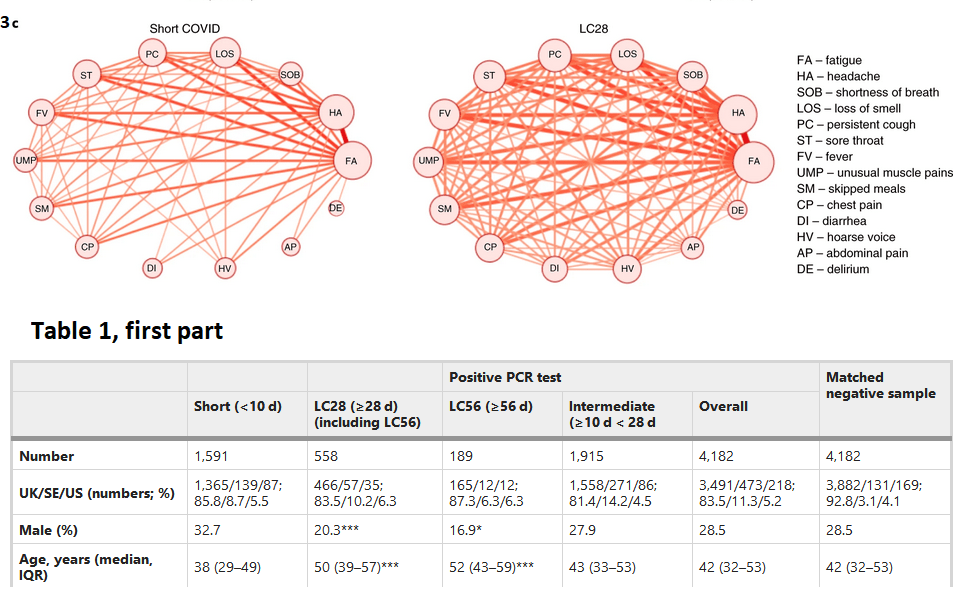
A study out of the UK published in April 2021 in Nature Medicine reported symptoms of patients suffering symptoms < 28 days, >28 day, >28 days, and >28 > 56 days. [12] Those that were hospitalized with short Covid or who had multiple short Covid symptoms were more likely to develop Long Covid. [12] Co-occurance of multiple symptoms is frequent in Lng Covid. Co-occurrence network of symptom pairs in which nodes represent symptoms, the frequency of symptoms corresponds to the size of the node, and the likelihood of symptom pair co-occurrence is represented by the weight of the edges linking them. Edges representing a co-occurrence of less than 10% were removed.
From reference [12] Almost 5% of the total Covid cases develop into symptoms that last more than 56 days.
Delirium seems to be associated with all other Covid sysymptoms in Long Covid.
Diarrhea (DI) and abdominal pain (AP) seem to require better definition as to the etiology if the primary infection has cleared. Is there permanent intestinal damage? If so, does this effect nutrient absorption?
Conclusions
It would appear that the scientific community has more hypotheses as to the cause of Long Covid than this post can even scratch the surface of. A few we have covered:
Active Covid-19 infections and Long Covid have similar symptoms.
Covid and autoimmune disease rheumatoid arthritis share common cytokines.
Exhausted T cells may play a roll in neurological issues of Long Covid. We don’t know if Cu(I)NA2 will be a cure for mitochondrial issues in T cells.
The Covid receptor ACE2 is widely expressed in the G.I. tract. It is conceivable that a short term consequence of an active Covid infection would be impaired absorption of copper.
Long Covid has an extremely large range of symptoms, many of which resemble the symptoms of current Mitosynergy customers.
Long Covid might be just four disorders, that have considerable overlap in terms of root cause.
It would be over speculative to suggest that Cu(I)NA2 supplies copper to one critical enzyme in any of these processes to cytochrome C oxidase in exhausted T cells to Cu/Zn superoxide dismutase trying to detoxify excess superoxide in the wake of autoimmune reactions. We can only point to similarities between Long Covid and the current Mitosynergy customer base.
Schett G, Manger B, Simon D, Caporali R. (2020) COVID-19 revisiting inflammatory pathways of arthritis. Nat Rev Rheumatol. 2020 Aug;16(8):465-470 PMC free article
Heming M, Li X, Räuber S, Mausberg AK, Börsch AL, Hartlehnert M, Singhal A, Lu IN, Fleischer M, Szepanowski F, Witzke O, Brenner T, Dittmer U, Yosef N, Kleinschnitz C, Wiendl H, Stettner M, Meyer Zu Hörste G.(2021) Neurological Manifestations of COVID-19 Feature T Cell Exhaustion and Dedifferentiated Monocytes in Cerebrospinal Fluid. Immunity. 2021 Jan 12;54(1):164-175.e6. PMC free article
DesdÃn-Micó G, Soto-Heredero G, Mittelbrunn M.(2018) Mitochondrial activity in T cells. Mitochondrion. 2018 Jul;41:51-57. PMC free article
Zhang H, Li HB, Lyu JR, Lei XM, Li W, Wu G, Lyu J, Dai ZM. (2020) Specific ACE2 expression in small intestinal enterocytes may cause gastrointestinal symptoms and injury after 2019-nCoV infection. Int J Infect Dis. 2020 Jul;96:19-24. PMC free article
Davis HE, Assaf GS, McCorkell L, Wei H, Low RJ, Reeme Y, Redfield S, Austin JP, Akrami A.Characterizing Long COVID in an International Cohort: 7 Months of Symptoms and Their Impact Cross Ref
Mahase E (October 2020). “Long covid could be four different syndromes, review suggests”. BMJ. 371: m3981. Cross Ref
Khamsi R. (2021) Rogue antibodies could be driving severe COVID-19. Nature. 2021 Feb;59 (7844):29-31. PMC free article
Stanculescu D, Larsson L, Bergquist J. (2021) Hypothesis: Mechanisms That Prevent Recovery in Prolonged ICU Patients Also Underlie Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Front Med (Lausanne). 2021 Jan 28;8:628029. PMC free article
Wood E, Hall KH, Tate W. (2020) Role of mitochondria, oxidative stress and the response to antioxidants in myalgic encephalomyelitis/chronic fatigue syndrome: a possible approach to SARS-CoV-2 ‘long-haulers’? Chronic Dis Transl Med. 2020 Nov 21. doi: 10.1016/j.cdtm.2020.11.002. PMC free article
Sudre CH et al (2021) Attributes and predictors of long COVID. Nat Med. 2021 Apr;27(4):626-631. PMC free article
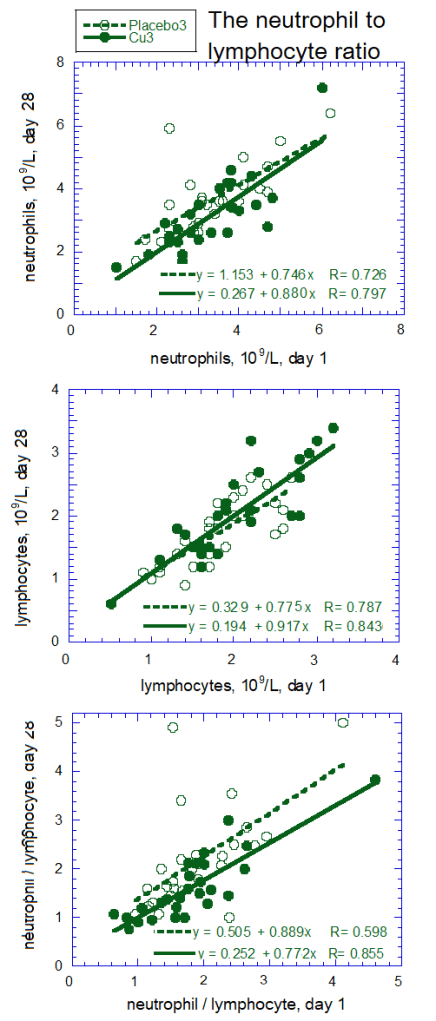
The importance of copper in the function of neutrophils and lymphocytes as been addressed on another post. This post never actually presented real data. We retrospectively analyzed data from a study performed by KGK Synergize in 2014. KGK analyzed the raw numbers of neutrophils and lymphocytes using an ANOVA model because the data were nonparametric. This post presents how we analyzed data collected by our CRO that has be registered at https://clinicaltrials.gov/ct2/show/NCT04737278. The graphs sort of tell their own story. Until FDA gives the green light, we are making no medical claims.
This free stats site uses six different sets for normality: Shapiro-Wilk, Shapiro-Francia, D’Agostino-Pearson, Jarque-Bera, Cramer-von Mises, Anderson-Darling. The sensitivity was set at p<0.05.
Given these results, it was decided to skip the ANCOVA in favor of ANOVA since the assumption of normality is met for NLR data. Went back and checked the neutrophil counts. Very definitely not a normal distribution.
Placebo1
Placebo2
Placebo3
Cu 1
Cu2
Cu3
Minimum
1.142857
0.958333
1
0.619048
0.625
0.766667
Maximum
3.727273
4.1
5
4.666667
4.6
3.833333
Sum
55.58982
53.29325
61.52245
49.65535
49.66772
45.39949
Points
28
28
28
28
28
28
Mean
1.985351
1.90333
2.19723
1.773405
1.773847
1.62141
Median
1.757143
1.745098
2.041667
1.666667
1.75
1.439103
RMS
2.091988
2.016828
2.410644
1.961878
1.927315
1.758534
Std Deviation
0.67149
0.679269
1.009854
0.854442
0.767495
0.693279
Variance
0.450899
0.461407
1.019805
0.730072
0.589048
0.480636
Std Error
0.1269
0.12837
0.190844
0.161474
0.145043
0.131017
Skewness
1.284053
1.271123
1.440843
1.756352
1.641878
1.399153
Kurtosis
0.920368
1.987952
1.794157
3.631511
4.685251
2.016536
normality
Pass all
Pass 1st 4
Pass all
Pass all
Pass all
Pass all
Placebo1-3 are NLR ratios on clinic visits 1-3 for the placebo group. Cu1-3 are NLR ratios for the Cu(I)NA2 group for clinic visits 1-3.
Having proven normal distribution another free stats website was used to perform ANOVA. A free site was used for 2-way ANOVA.
ANOVA Summary
Source
SS
df
MS
F
p
visits
0.41
1
0.41
0.65
0.422
treatments
3.26
1
3.26
5.14
0.025
visits x treatments
1.31
1
1.31
2.07
0.153
Error
66.57
105
0.63
Total
71.55
108
A table of Anova values from teh free website. Note that only the treatment term is significant.
Placebo
Cu(I)NA2
P Value
Mean ± SD (N) Median (Min – Max)
Mean ± SD (N) Median (Min – Max)
Neutrophils (109/L)
Screening
3.49 ± 1.12 (28) 3.4 (1.8 – 6.4)
3.45 ± 1.16 (28) 3.2 (1.3 – 6.3)
–
Baseline
3.35 ± 1.13 (28) 3.1 (1.5 – 6.2)
3.28 ± 1.06 (28) 3.15 (1 – 6)
–
Visit 3 (Day 28)
3.60 ± 1.13 (27) 3.6 (1.7 – 6.4)
3.15 ± 1.19 (26) 2.85 (1.5 – 7.2)
0.03*
Change from Baseline to Visit 3
0.32 ± 0.83 (27) 0.2 (-0.8 – 3.6) p = 0.05§
-0.13 ± 0.73 (26) 0.05 (-1.9 – 1.2) p = 0.38§
–
Lymphocytes (109/L)
Screening
1.84 ± 0.51 (28) 1.9 (0.8 – 2.8)
2.15 ± 0.69 (28) 2.15 (0.6 – 3.4)
–
Baseline
1.83 ± 0.51 (28) 1.8 (0.9 – 2.7)
2.01 ± 0.64 (28) 1.9 (0.5 – 3.2)
–
Visit 3 (Day 28)
1.74 ± 0.51 (27) 1.8 (0.9 – 2.6)
2.04 ± 0.72 (26) 2 (0.6 – 3.4)
<0.01*
Change from Baseline to Visit 3
-0.08 ± 0.34 (27) 0 (-0.8 – 0.4) p = 0.22§
0.03 ± 0.39 (26) 0.1 (-0.8 – 1) p = 0.73§
–
Neutrophil to lymphocyte ratio
Screening
1.99 ± 0.67 1.76 (1.14-3.72)
1.77 ± 0.85 1.67 (0.62-4.57)
Baseline
1.90 ± 0.68 1.75 (0.96-4.1)
1.77± 0.77 1.75 (0.625-4.6)
p=0.44§
Visit 3 (Day 28)
2.20 ± 1.03 2.08 (1.0-5.0) p=0.066§
1.62 ± 0.69 1.44 (0.77-3.83) p=0.054§
p=0.03∆
Change from Baseline to Visit 3
-0.294 ± 0.813 -0.049 -3.38 to 1.38
0.152 ± 0.400 0.123 -0.625 to 0.902
p<0.05§
Table 3 Changes in white blood cell populations indicative of inflammatory status. *Between group comparisons were made using ANCOVA. §Within group comparisons were made using the paired Student t-test. Probability values ≤0.05 are statistically significant. ∆ 2 way ANOVA treatment effect Note change from baseline to visit 3 is positive if there is a decrease in the cell count or a decrease in the ratio.
Note that a change in baseline to Visit 3 is the baseline value minus the Visit 3 value. A The mean change in baseline to visit 3 decreased in the placebo group meaning that the NLR increased in the placebo group.
Examples of Cu(I)NA2 helping those that are..
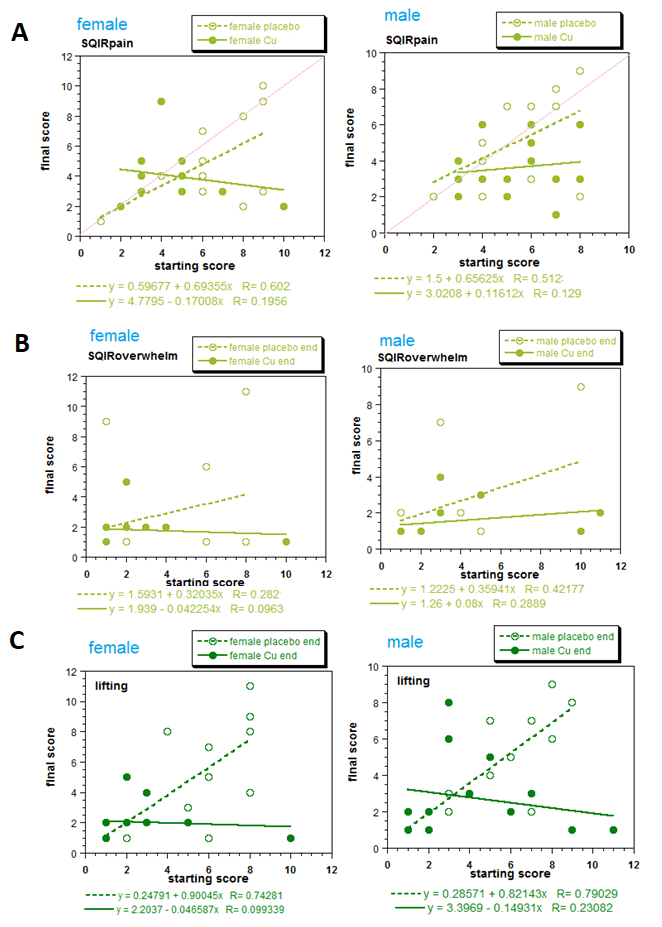
Mitosynergy has a conviction that customers that are worse off have the most symptom improvement. This multiple regression model provides preliminary statistical backing for this conviction. The red line of “manuscript in preparation Figure 4A illustrates what one would see if there was no improvement of the baseline score on the X-axis to the score on day 28 on the Y-axis. The slope would be 1.0. The equation of a line documenting a complete “cure” would have a slope of 0 and and a Y-intercept of 0 to 1. The placebo slopes were about 0.65, close enough to 1.0. The slopes of theCu(I)NA2 line for the females was less than 0, -0.17. Examination of the NLR will reveal a different phenomenon.
Figure 4 (a manuscript in progress) Exemplary graphs from SQIR questions A. Symptom Domain, pain. In females the probability is higher that the Cunermuspir and placebo lines have different slopes (p=0.037). In males the probability that the lines have different slopes did not meet the threshold of significance. Red lines indicate the slope of 1.0, or no change in the score from baseline to day 28. B. Impact Domain, overwhelm by symptoms. C. Function Domain, lifting bags of groceries. For both males and females the slopes of the Cunermuspir and placebo lines are different at p=0.0114 and p= 0.0043, respectively.
A graphical view of the NLR
Figure 5 Neutrophils, lymphocytes, and the neutrophil /lymphocyte ratios: the amount on day 28 as a function of baseline, day 1.
Male and female data were combined when analyzing neutrophil and lymphocyte counts because separating the data did not reveal any difference. Population variations are very apparent when the data are presented graphically. The interesting phenomenon is that the slopes of the lines of the placebo and Cu(I)NA2 were statistically the same. The y-intercepts appear to be different. While these small studies are to be interpreted with caution, Cu(I)NA2 seems to improve the NLR ratio for all the participants a little.
Inspired by Coronavirus 2019 (COVID-19)- Using Ascorbic Acid and Zinc Supplementation (COVIDAtoZ)
This study protocol differs from other iterations as the Covid-19 death toll reaches 400,000. There’s a nice zinc supplement study zinc supplement study: A single-center, prospective, open label four arm study (1. Zinc only 2. Zinc and ascorbic acid 3. Ascorbic acid only 4. Standard of care.
Looking Back, comparing two coppers on immune parameters in chickens
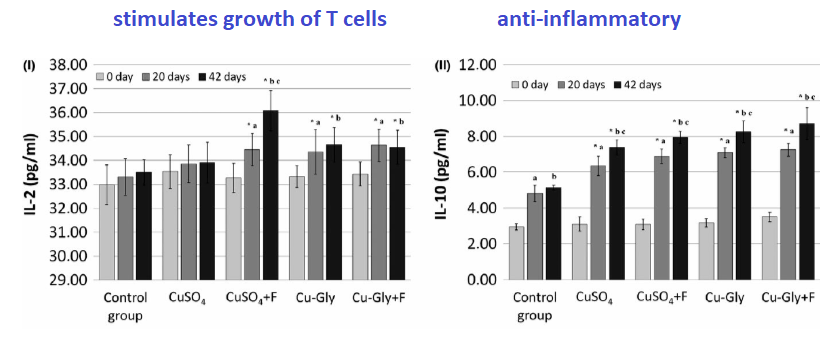
The updated plan would be to perform blood draws only after the patient has a negative PCR test. Time to negative PCR test will be a new outcome measure. By restricting blood draws, money could be saved towards including an active comparatar rather than a placebo. Cupric glycinate is one such active compound (Jarosz 2018). These authors tested the hypothesis that Cu(II)Gly could improve cell based (T cell lineages) and humoral (cytokine) immune parameters in boiler chickens. These authors also included the plasma based copper carrier protein ceruloplasmin and erythrocyte Cu/Zn superoside dismutase (SOD) in their analyses. Chickens were treated with two forms of cupric copper (CuSO4 and Cu(II)Gly) phytase (F) A phytase (myo-inositol hexakisphosphate phosphohydrolase) is any type of phosphatase enzyme that catalyzes the hydrolysis of phytic acid (myo-inositol hexakisphosphate) – an indigestible, organic form of phosphorus that is found in many plant tissues. The roosters were suplemented wtih 16 mg Cu per kg feed in addition to the normal requirements for Ross 308 broiler chickens.
Data were analyzed with the Kruskal Wallis non-parametric version of the t-test. * different from the control (p<0.05) a different from day 0 to day 20 b different from day 0 to day 42 c different from cay 20 to day 42
Note that cupric glycinate out performs CuSO4. The way the data were presented, it is kind of hard to tell if the phytase enzyme did any good. These authors also looked at Interleukin 2 (IL-2) and IL-10. Both copper compounds greatly increased IL-10 from day 20 to day 42.
Data were analyzed with the Kruskal Wallis non-parametric version of the t-test. * different from the control (p<0.05) a different from day 0 to day 20 b different from day 0 to day 42 c different from cay 20 to day 42
Lymphocyte sub populations
These authors characterized lymphocytes (immune cells associated with antibody production) based on surface markers. CD3+ is a T-cell marker. CD4+ marks the cell as a T helper cell. CD8+ marks a T cell as a a cytotoxic T cell that are best known for killing cancer cells. CD25 is the IL-2 receptor. It is found on activated T and B cells. MHC class II are surface proteins that present antigens on macrophage and dendritic cells, to name a few. Bu-1a is an antigen found on bursal cells of one day old hens.The Bursa of Fabricius is a lymphoid organ found only in birds
CD3+CD4+ Phytase and Cu-Gly seemed to have elicited the biggest increases in the CD4+ sub population.
CD3CD8+ Only copper glycinate with phytase increased this marker at day 42.
CD25+ Cu-Gly increased the IL-2 receptor positive cells on day 20 and 42 compared to day 0. Phytase was not reported to increase IL-2 receptor presence.
MHC class II Cu-Gly, with and without phytase, increased the percent positive on days 20 and 42 compared to day 0.
Bu-1a Both copper supplements result in significant (p<0.05) but slight increases in this antigen marker. Phytase did not seem to do much.
The take home is that the type of Cu(II) made a difference in the immune systems in these boiler chickens.
Looking forward, Comparing types of copper in humans
The eye opening and worthy of emulation thing is that they expose no laboratory to personnel to Covid. It might also cut down on cost for C LAB Pharma if we only do blood work on day 28. Also, having an IRB working with us from the start will probably save time in the long run.
These are some proposed arms of a Covid study
2 mg Cu per day, 6 mg Cu 48 hours pyrexia in the form of Cu(I)NA2
2 mg Cu per day, 6 mg Cu 48 hours pyrexia in the form of Cu(II)glycinate
Covid-19 standard of care
Reference
Jarosz ÅS, Marek A, GrÄ…dzki Z, KwiecieÅ„ M, Kaczmarek B. The effect of feed supplementation with a copper-glycine chelate and copper sulphate on selected humoral and cell-mediated immune parameters, plasma superoxide dismutase activity, ceruloplasmin and cytokine concentration in broiler chickens. J Anim Physiol Anim Nutr (Berl). 2018 Feb;102(1):e326-e336. doi: 10.1111/jpn.12750. Epub 2017 Jun 12. PMID: 28603872.
This post started in the Fall of 2020 when one of us had a little dog with a very bad resurgence of Valley Fever, aka Coccidiodomycosis. The little dog went back on Fluconazole and some carprofen for the “pain” a not so good vet insisted she was in. This same vet wanted to amputate the front right leg at the shoulder joint. The carprofen made the poor little dog woozy. She fell down half a flight of stairs and injured her back. We put her on some Mitosynergy Cu(I)NA2 and hemp oil on top of the Fluconazole.
Last Fall the little dog could not use her right front leg due to joint damage to the shoulder. This was before the Valley fever went away and came back with a vengeance. She can now use all four legs to walk. Was it the Fluconazole, the copper, the hemp oil, or a combination? This post explores how copper is handled by some select fungi. Please feel free to share this post with your pet’s veterinarian. Do not under any circumstance use this post to play games with your pet’s health without a veterinarian’s assistance! Coccidiodomycosis can kill your pet! Some vets say that a dog must be on Fluconazole for life if there is joint damage no matter how low the antibody titers.
Back to the original post
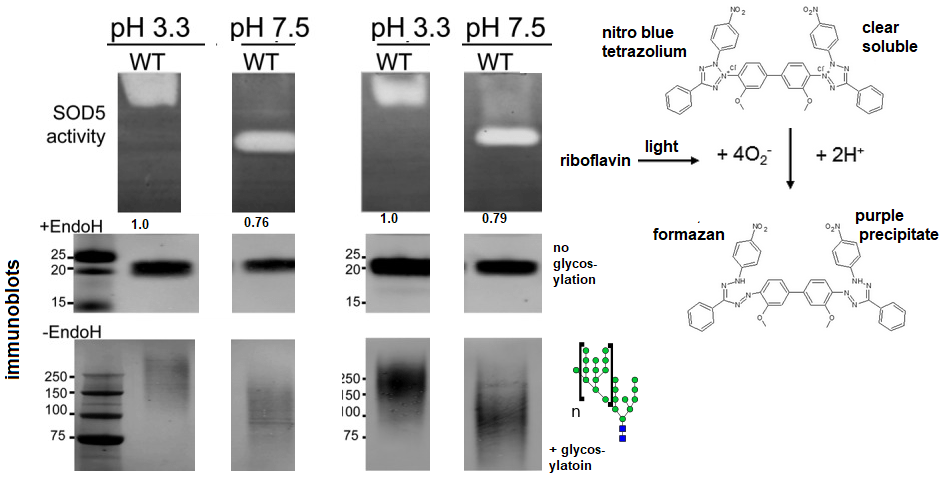
Unlike mammalian SOD1 and SOD3, The Candida albicans SOD5 only binds copper and is a monomer rather than a dimer [1]. In addition, the copper site of SOD5 is solvent accessible. This will become important keeping copper that enters the mammalian body reserved for our SOD rather than that of a pathogenic yeast or fungi. Peterson and coworkers found that SOD5’s activity decreased above pH 7.5. [1]. these authors were also concerned with how key amino acids controlled this pH dependency. They were also concerned with how the pH of the growth of the medium controlled expression of SOD5. Duplicate experiments in Figure 1 show that that SOD5 expressed at pH 3.3 is slightly more active than that expressed at pH 7.5. Glycosylation, attachment of polymeric sugar residues is also more robust at pH 7.5. Anionic proteins in native gels migrate to the negatively charged anode. The addition of sugar residues in the form of glycosylation increases their migration towards the bottom of the gel. Note that the enzyme assays in the native blue tetrazolium gels was performed with full glyosylation, i.e. no EndoH to remove the sugars.
Fig. 1Top left SOD5 activity as a function of growth conditions. Experiments were presumably preformed in duplicate. Numbers under the gels represent relative intensity of the white bands. Bottom Left Immunoblots with and without ENdoH enzyme treatment to remove glycosylation. Right SOD acitivity is detected by generation of supreoxide by exposing riboflavin to light. Superoxide, O2-, is generated by this reaction. O2– reacts with nitro blue tetrazolium to form a purple precipitate in the gel.
SOD5 to escape host super oxide attack
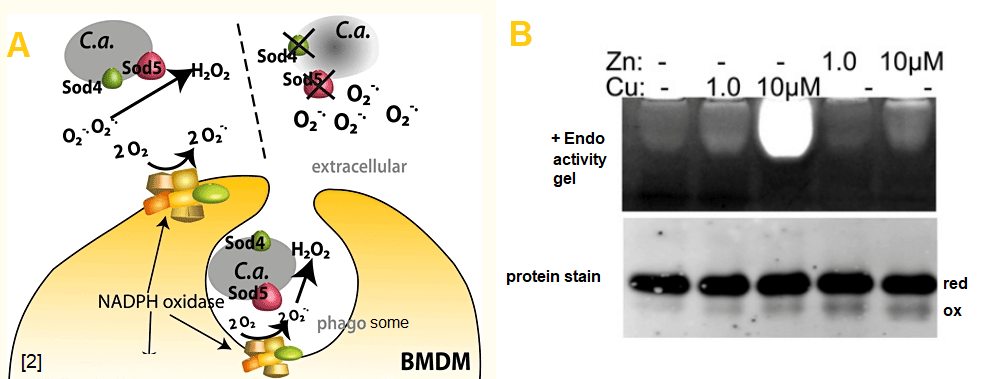
Candida albicans lacking SOD5, but not SOD6, are more susceptible to superoxide induced killing by co-culture with bone marrow derived macrophage (BMDM). [2] Unlike mammalian Cu/Zn SOD 1/2, SOD5 is not loaded with copper by chaperones, it acquires copper from the host’s extracellular spaces. [3]. This particular reference goes into structural aspects of an intra chain disulfide bond. Intra chain disulfide bonds can make a protein more compact such that they appear to run faster in a gel.
Fig. 2A General mechanism by which SOD5 protects C albicans from host superoxide attack [3] B From reference [3] SOD5 acquires copper from the extracellular environment for activity. Zince has no effect on activity. An intrachain disulfide bond may be reduced (red) or oxidized (ox)
Because SOD5 is loaded with copper from extracellular spaces of the host, that is to say blood, it makes sense that chelators may be used to remove this copper [4]. The ideal chelator will remove copper from SOD5 but not Cu/Zn SOD1/3. Mitosynergy has a different and more natural strategy. Mitosynergy is of the opinion that copper in the +1 oxidation state will be absorbed differently than copper in the +2 oxidation state. Proper absorption is predicted to fuel host Cu/Zn SOD 1/3 while leaving yeast SOD5 starved for copper.
References
Peterson RL, Galaleldeen A, Villarreal J, Taylor AB, Cabelli DE, Hart PJ, Culotta VC.(2016) The Phylogeny and Active Site Design of Eukaryotic Copper-only Superoxide Dismutases. J Biol Chem. 2016 Sep 30;291(40):20911-20923. [PMC free article]
Gleason J. E., Galaleldeen A., Peterson R. L., Taylor A. B., Holloway S. P., Waninger-Saroni J., Cormack B. P., Cabelli D. E., Hart P. J., and Culotta V. C. (2014) Candida albicans SOD5 represents the prototype of an unprecedented class of Cu-only superoxide dismutases required for pathogen defense. Proc. Natl. Acad. Sci. U.S.A. 111, 5866–5871 10.1073/pnas.1400137111 [PMC free article]
Frohner IE, Bourgeois C, Yatsyk K, Majer O, Kuchler K.(2009) Candida albicans cell surface superoxide dismutases degrade host-derived reactive oxygen species to escape innate immune surveillance. Frohner IE, Bourgeois C, Yatsyk K, Majer O, Kuchler K. Mol Microbiol. 2009 Jan;71(1):240-52. [PMC free article]
Robinett NG, Culbertson EM, Peterson RL, Sanchez H, Andes DR, Nett JE, Culotta VC.(2019) Exploiting the vulnerable active site of a copper-only superoxide dismutase to disrupt fungal pathogenesis. J Biol Chem. 2019 Feb 22;294(8):2700-2713. [PMC free article]