We have heard about IL-1 as part of the Covid-19 cytokine storm. It is often labeled as a bad player in many varieties of inflammation. IL-1 is actually a family of small proteins, IL-1β being the most notorious, pro-inflammatory member. IL-1β is part of many inflammatory diseases. This post is not intended to offer medical advise but rather to give busy MDs some background information to continue their educations.
In a 1989 study looked at human rheumatoid arthritis patients who had relatively high levels of the copper/iron carrier ceruloplasmin but not erythrocyte Cu/Zn superoxide dismutase activity. Activity levels of Cu/Zn SOD increased after 4 weeks of copper supplementation (2 mg/day). For obvious reasons, the Cu/Zn SOD activity of inflamed tissues was not investigated. Cell cultured experiments with human fiborblasts revealed thatinterleukin-1 elevated Cu-Zn SOD activities in cultured fibroblasts.
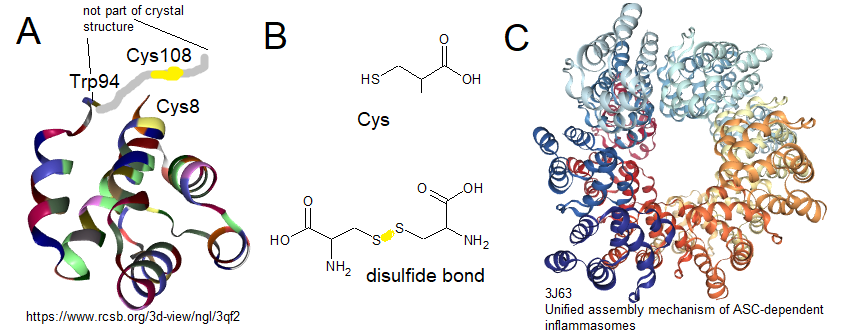
IL-1 is produced by inflammasomes, protein assemblies that contain a protein called NLRP3/NALP3. In 2011 Bae and Park identified a disulfide bond between Cys8 and Cys108. The last few amino acids, of which was Cys108, were not resolved in this crystal structure.
fff
A. From Bae and Park, crystal structure of pyrin domain of NLRP3. A hypothetical portion of the domain from Trp94 to the C-terminus is scribbled in. While not in the crystal structure Cys8 and Cys108 can form disulfide bonds B Cysteine (Cys) can form disulfide bonds with other Cys. C. NLRP3 pyrin domains can bind to each other or pyrin domains in ASC.
fff
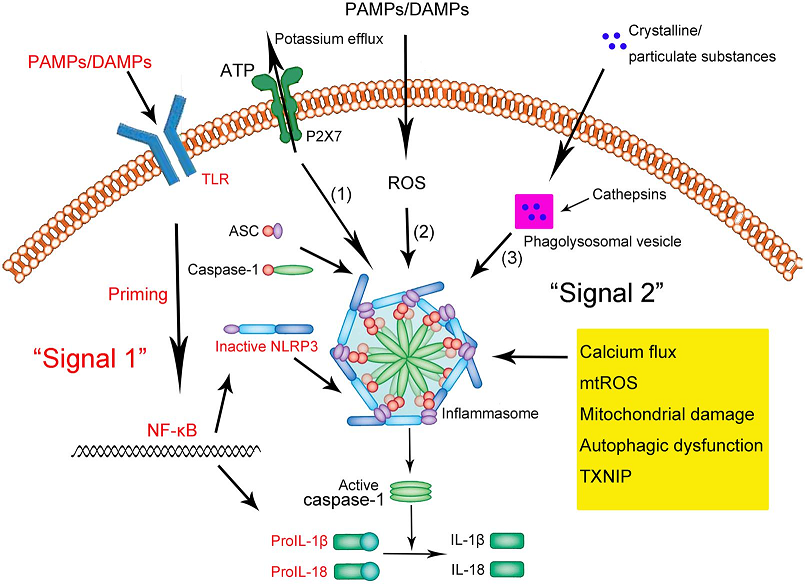
Figure 1 from the Shao [1] Review.
Gram negative lipopolysaccharide, pathogen and danger associated molecular patterns (PAMP. DAMP), and such may be recognized by TLR4, which signals the nucleus to produce more inactive IL-1, NLRP3, and so on [2].
Particular irritants from inorganic particles to beta amyloid deposits may be phagocytosed. When these phagosomes rupture, the protease cathepsin, and assorted irritants are released into the cell.
Finally, reactive oxygen species may trigger inflammasome assembly.
In addition to containing the pyrin domain with the redox sensitive disulfide bond, the NLRP3 protein belongs to the family of nucleotide-binding and oligomerization domain-like receptors (NLRs)[2]
Adapter protein apoptosis-associated speck-like protein (ASC) A variety of signals cause NLRP3 to open up and bind ASC. This complex activates
Procaspase-1 (green ellipse) is an and self inhibited inactive protease. Binding to the NLRP3/ASC complex allows self digestion of the inhibitor portion (rose circle)
Active caspase-1 cleaves inactive proIL-1β to an active cytokine.
The paradoxical role of Cu/Zn SOD1
Chelation therapy not so fast!
Deigendesch and coworkers tested the hypothesis that copper causes inflammation. These authors demonstrated that NLRP3 inflammasome activation is blocked by removing copper from the active site of superoxide dismutase 1 with the copper chelator tetrathiomolybdate, [4] Inflammasome function is also impaired in Cu/Zn SOD deficient mice. Copper regulation was found in macrophages, but not monocytes, both in mice and humans. Chelation of bioavailable copper resulted in attenuated caspase-1–dependent inflammation. The authors reported reduced susceptibility to LPS-induced endotoxic shock. Because the chelator tetrathiomolybdate is clinically used to treat Wilson’s Disease, it might prove useful in inflammatory diseases involving the NLRP3 inflammasome.
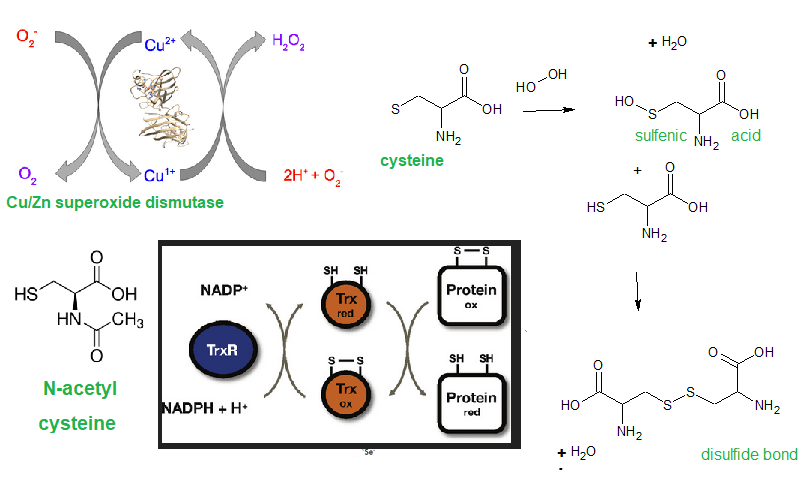
Top left, Cu/Zn SOD produces hydrogen peroxide as a byproduct. H2O2 reacts with cysteine to produce cysteine sulfenic acid. Cysteine sulfenic acid reacts with reduced cysteine to produce a disulfide bond. Thioredoxin (Trx) restores protein disfuldide bonds to their reduced state.
Hydrogen peroxide has been described as a signalling molecule, or second messenger (5]. This disulfide bond of NRLP3 could be dependent on H2O2 from superoxide dismutase. While H2O2 reacts with thiols, it really is not as damaging as super oxide. Catalase also depletes hydrogen peroxide: H2O2 → 2 H2O + O2
The thiol of cysteine in proteins may form disulfide bonds with other protein scyteine thiols or with a low molecular weight thiol (PSSR, where R is anything and P is a protein. ) Any reduced low molecular weight thiol compound (R’SH) can take things back to normal.
protein − SSR + R′SH ⇄ protein − SH + RSSR′ [5]
Could N-acetyl cysteine be a source of reducing equivalents like the protein thioredoxin? Indeed, copper and N-acetyl cysteine have been suggested as therapies for Covid-19 in conjunction with standard treatments [6]
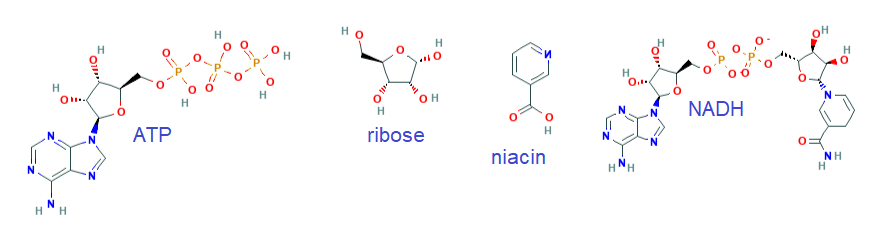
And finally, what about the niacin in Cu(I)NA2? Could niacin be a precursor for more NADH + H+ that provides thioredoxin with reducing equivalents to inactivate the IL-1β producing inflammasome?
Niacin can be a precursor for NADH, a small molecule that supplies reducing equivalents to thioredoxin, and many other things
If you are a physician thinking about putting your patient on a chelation therapy to reduce inflammation… maybe not so fast. We need Cu/Zn SOD to scavenge super oxide. H2O2 is a less reactive messenger that tells the body there’s trouble via inflammasomes and IL1β. Your patient just needs reducing equivalents to turn the inflammasome off after it’s done it’s job.
References
DiSilvestro RA. (1989) Effects of inflammation on copper antioxidant enzyme levels.Adv Exp Med Biol. 1989;258:253-8
Bae JY , Park HH (2011) Crystal structure of NALP3 protein pyrin domain (PYD) and its implications in inflammasome assembly J Biol Chem 286(45):39528-36. [PMC free article]
Shao BZ, Xu ZQ, Han BZ, Su DF, Liu C. (2015) NLRP3 inflammasome and its inhibitors: a review. Front Pharmacol. 2015 Nov 5;6:262 [Cross Ref]
Deigendesch N, Zychlinsky A, Meissner F. (2018) Copper Regulates the Canonical NLRP3 Inflammasome. J Immunol. 2018 Mar 1;200(5):1607-1617. [PMC free article]
Forman HJ, Maiorino M, Ursini F.(2010) Signaling functions of reactive oxygen species. Biochemistry. 49(5):835-42. [PMC free article]
Andreou A, Trantza S, Filippou D, Sipsas N, Tsiodras S. (2020)COVID-19: The Potential Role of Copper and N-acetylcysteine (NAC) in a Combination of Candidate Antiviral Treatments Against SARS-CoV-2. In Vivo. 2020 Jun;34(3 Suppl):1567-1588 [Cross Ref]
Freeman TL, Swartz TH. (2020) Targeting the NLRP3 Inflammasome in Severe COVID-19. Front Immunol. 2020 Jun 23;11:1518. [PMC free article]
Coivd-19 patients have difficulty breathing. Is this due to lost of lung capacity, the cytokine storm, or a combination of the two? The neurons of the locus ceruleus are themselves very sensitive to CO2/pH. [1] The A6 norepinepthrine releasing neurons of the LC play a role in translating changes in CO2/pH to changes in respiration. [2] This post started asking if cytokines in the Covid-19 cytokine storm effect neurons in the locus ceruleus.
From the peritoneum to the brain
Borsody and Weiss(2005) followed up on previous studies that demonstrated that ip injection of microbial substances–
increased the spontaneous discharge rates and sensory-evoked responses of isolated locus coeruleus (LC) neurons in a dose- and time-related manner in rats. Complete transection of the subdiaphragmatic vagus nerves abolished this response. A variety of microbial substances excited LC neurons after administration into the peritoneal cavity in a manner involving the subdiaphragmatic vagus nerves.[3] Perhaps these studies have ramifications of any bacterial or viral sepsis.
IL-1
Both i.p. peptidoglycan and poly(I)/(C) increased LC activity but with lesser efficacy than LPS. Â Was this due to the inflammatory cytokine interleukin 1 (IL-1)? IL-1 receptor antagonists ( IL-1RA) reversed the increase in the activity of LC neurons caused by i.p. peptidoglycan treatment; however, that caused by i.p. Poly(I)/(C) was not diminished by IL-1RA. Thus, the increased activity of LC neurons caused by LPS and peptidoglycan requires IL-1 receptor binding, suggesting the involvement of endogenously-produced IL-1. In contrast, poly(I)/(C) increased the activity of LC neurons but this did not critically involve IL-1 receptors in the LC. [4].
IL-2
Receptors for interleukin 2 are generally considered to be expressed in memory and regulatory T cells. The early 1990s saw interest in the neuro-immune axis. De Sarro and Nisticó injected recombinant human and rat IL-2 into the locus ceruleus of rat brains and measured electrical activity. [5]. IL-2 injection caused slow wave sleep like patterns that were disrupted by agents that inhibit the heterotrimeric G protein signalling that is used by many cytokines receptors as well as cannabinoid receptors [5]
IL-6 in combination with IL-1
Ventricles of mice were injected with interleukin IL-1β (0.5 μg) and IL-6 (1 μg) [6] IL-1β and IL-6-dependent LC neuronal activation induced depression-like behavior and IL-1β induced increase in leptin levels enhanced α1-adrenoceptor-mediated depression-like behavior.
IL-7 and IL-10
Not addressed directly in the literature, i.e. PubMed searches.
IP-10 aka Cxcl 10
Cxcl-10 in an interferon gamma induced secreted protein that is a well established component of the Covid-19 cytokine storm. [7]Â Cxcl 10 has also been speculated to be responsible for loss of taste and smell in Covid-19 infections.
 GM-CSF
Granulocyte-macrophage colony-stimulating factor is being explored as a therapeutic target for Coivd-19 via antibodies against this secreted pro-inflammatory cytokine as well as its receptor [8]. Myeloid cells activated by GM-CSF may secrete inflammatory cytokines IL-1 and IL-6 as well as reactive oxygen species. [8] IFNγ prevents secretion of GM-CSF and fatal HSV1 encephalitis caused by the invasion of the brain stem by inflammatory monocytes and neutrophils [9].
MCP-1, aka CCL2
(TNF-α), chemokine (C-C-motif) ligand 2 (CCL2), and granulocyte-macrophage colony-stimulating factor (GM-CSF). A recent review lists these cytokines as part of the COVID-19 cytokine storm: IL-6)\, IL-1β, TNF-α, GM-CSF, and CCL2. [10] The Kempurai does a nice job of reviewing the Covid-19 virus and the cytokine storm. Then the authors discuss locus ceruleus psychological aspects of Covid-19 such as
tension that can increase shortness of breath
sleeping disorders
fear and anxiety
Another story found that patients with mood disorders or suicide attempt were more likely to be sero positive for Coivd-19 and influenza A and B viruses. [11]Â The effect of viral associated cytokines on expression of enzymes involved in serotonin synthesis was speculated to be be part of the iteology. [11]
MIP-IA
Macrophage inflammatory protein (MIP-1) may also induce the secretion of IL-1, IL-6, and TNFα .
TNFα,
Keneko and coworkers [12] injected mice with lipopolysaccharide and found that this stimulated microglial cells to produce TNF-α. They also found that NE from the locus ceruleus suppressed this inflammatory response. The influence on respiration was not addressed.
H5N1 and ventilation
The highly pathogenic H5N1 (HK483) viral infection causes a depressed hypercapnic ventilatory response (dHCVR, 20% ↓) at 2 days post infection (dpi) and death at 7 dpi in mice The authors cited four centers of the ventilation in repose to hypoxia and/or elevated CO2
 Glomus cells in the carotid body.  Viral nucleocapsid protein NP was not found at this site.
NE secreting neurons in locus coeruleus (LC). These neurons are sensitive to local acidosis. Viral NP was found in 35% of tyrosine hydroxylase posititive neurons.
In serotonergic neurons in the raphe nuclei, 10% of the tryptophan hydrolase expressing neurons were also positive for viral NP.
The neurokinin 1 receptor (NK1R)-expressing neurons in the retrotrapezoid nucleus (RTN) are chemosensitive and responsible for HCVR. Viral NP was found in 20% of the neurons.
The authors asked whether the dHCVR became worse over the infection period with viral replication in these cells/neurons. Mice intra nasally inoculated with saline or the HK483 virus were exposed to hypercapnia for 5 min at 0, 2, 4, or 6 dpi, followed by immunohistochemistry to determine the expression of nucleoprotein of H5N1 influenza A (NP) alone ….[13]
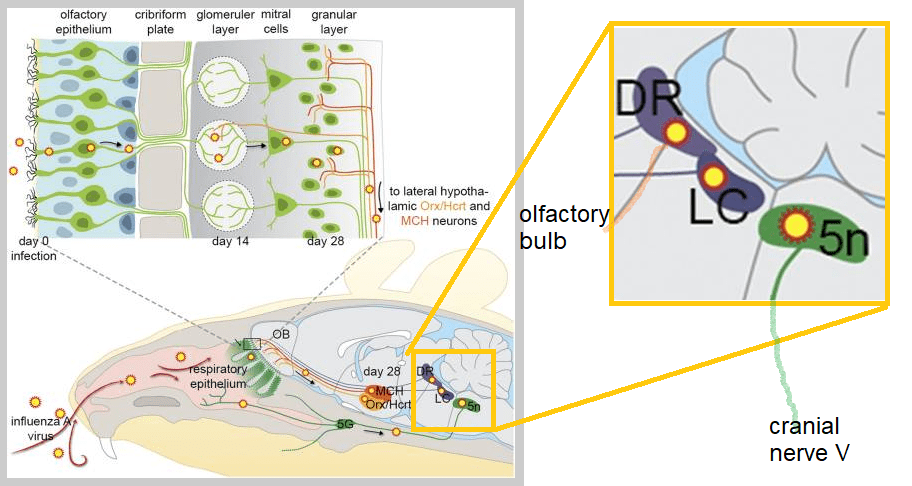
Mice lacking the used mice with a targeted deletion of the Recombinant activating gene 1 (Rag1−/− )  lack functioning T and B cells. They can mount an innate but not adaptive immune response against the H1N1 virus. A 2016 study out of the Karolinska Institute tested the hypothesis that the H1N1 virus could lead to narcolepsy like symptoms in immune compromised rats.  These authors discussed the autoimmune like loss of orexin secreting neurons in the lateral hypothalamus and the possible role of the H1N1 vaccine.
When the nasal passages of the mice were inoculated with H1N1, sleep/wake disturbances followed in a few weeks. [14]Â These authors observed viral infection of the noradrenergic neurons of the locus ceruleus. [14]
Â
Adaped from Figure 6 of reference [14] The neural invasion of H1N1 into the brains of immuno compromised mice. The Dorsal Rpahe nucleus has projections to the olfactory bulb and amygdalla. The locus ceruleus (LC) affects respiration and sleep/wake cycles. The trigeminal nerve projects to cranial nerve V.
References
de Carvalho D, Patrone LG, Taxini CL, Biancardi V, Vicente MC, Gargaglioni LH. (2014) Neurochemical and electrical modulation of the locus coeruleus: contribution to CO2drive to breathe. Front Physiol. 2014 Aug 5;5:288. [PMC free article]
Magalhães KS, Spiller PF, da Silva MP, Kuntze LB, Paton JFR, Machado BH, Moraes DJA. (2018) Locus Coeruleus as a vigilance centre for active inspiration and expiration in rats. Sci Rep. 2018 Oct 23;8(1):15654. [PubMed free article]
Borsody MK, Weiss JM.(2005) The subdiaphragmatic vagus nerves mediate activation of locus coeruleus neurons by peripherally administered microbial substances. Neuroscience. 2005;131(1):235-45
Borsody MK , Jay M Weiss JM (2004) The effects of endogenous interleukin-1 bioactivity on locus coeruleus neurons in response to bacterial and viral substances Brain Res 1007(1-2):39-56.
De Sarro G, Nisticó G. (1991) Effects of pertussis toxin, dibutyryl-cyclic-AMP, bromo-cyclic-AMP and forskolin on the behavioural and electrocortical power spectrum changes induced by microinfusion of interleukin-2 into the locus coeruleus. Int J Neurosci. 1991 Jul;59(1-3):67-79
Kurosawa N, Shimizu K, Seki K(2016) The development of depression-like behavior is consolidated by IL-6-induced activation of locus coeruleus neurons and IL-1β-induced elevated leptin levels in mice. Psychopharmacology (Berl). 2016 May;233(9):1725-37.
Oliviero A, de Castro F, Coperchini F, Chiovato L, Rotondi M. (2020) COVID-19 Pulmonary and Olfactory Dysfunctions: Is the Chemokine CXCL10 the Common Denominator? Neuroscientist. 2020 Jul 13:1073858420939033. [Cross Ref]
Lang FM, Lee KM, Teijaro JR, Becher B, Hamilton JA. (2020) GM-CSF-based treatments in COVID-19: reconciling opposing therapeutic approaches. Nat Rev Immunol. 2020 Jun 23:1-8 [PMC free article]
Ramakrishna C, Cantin EM. (2018) IFNγ inhibits G-CSF induced neutrophil expansion and invasion of the CNS to prevent viral encephalitis. PLoS Pathog. 2018 Jan 19;14(1):e1006822. [PMC free article]
Kempuraj D, Selvakumar GP, Ahmed ME, Raikwar SP, Thangavel R, Khan A, Zaheer SA, Iyer SS, Burton C, James D, Zaheer A. (2020) COVID-19, Mast Cells, Cytokine Storm, Psychological Stress, and Neuroinflammation. Neuroscientist. 2020 Jul 18:1073858420941476 [Cross Ref]
Okusaga O, Yolken RH, Langenberg P, Lapidus M, Arling TA, Dickerson FB, Scrandis DA, Severance E, Cabassa JA, Balis T, Postolache TT.(2011) Association of seropositivity for influenza and coronaviruses with history of mood disorders and suicide attempts. Version 2. J Affect Disord. 2011 Apr;130(1-2):220-5. [PMC free article]
Kaneko YS, Mori K, Nakashima A, Sawada M, Nagatsu I, Ota A. (2005)Peripheral injection of lipopolysaccharide enhances expression of inflammatory cytokines in murine locus coeruleus: possible role of increased norepinephrine turnover. J Neurochem. 2005 Jul;94(2):393-404. [PMC free article]
Zhuang J, Zang N, Ye C, Xu F.(2019)Lethal avian influenza A (H5N1) virus replicates in pontomedullary chemosensitive neurons and depresses hypercapnic ventilatory response in mice. Am J Physiol Lung Cell Mol Physiol. 2019 Mar 1;316(3):L525-L536.[PMC free article]
Tesoriero C, Codita A, Zhang MD, Cherninsky A, Karlsson H, Grassi-Zucconi G, Bertini G, Harkany T, Ljungberg K, Liljeström P, Hökfelt TG, Bentivoglio M, Kristensson K.(2016) H1N1 influenza virus induces narcolepsy-like sleep disruption and targets sleep-wake regulatory neurons in mice. Proc Natl Acad Sci U S A. 113(3):E368-77. [PMC free article]
Do temperatures associated with infections track diurnal variations of body temperatures?Â
A trip back to the 1800s
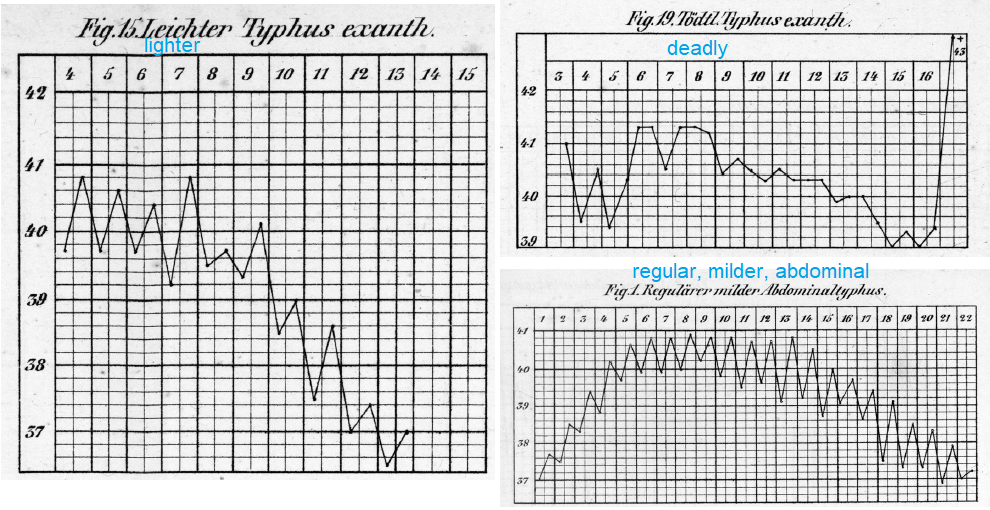
Sometimes searching for images is a good way of finding things.  One such image search led us to an article in a journal called the History of Science[1]. The authors described a group of physicians turning their clinics into a laboratory. The physicians recorded the temperature of typhoid fever patients twice a day. Note that in Figure 19, the patient that died with a fever over 43oC, 109.4oF. Also note that the other patients had daily high and low temperatures.
Fig 1 Specific temperature curves of typhus and typhoid fevers. From C. A. Wunderlich, Das Verhalten der Eigenwärme in Krankheiten (Leipzig, 1868). See reference[1]This publication seems to have inspired a Russian language account of the same phenomenon. We do not know if this is the abdominal variety, but the temperature curve sure presents that way.
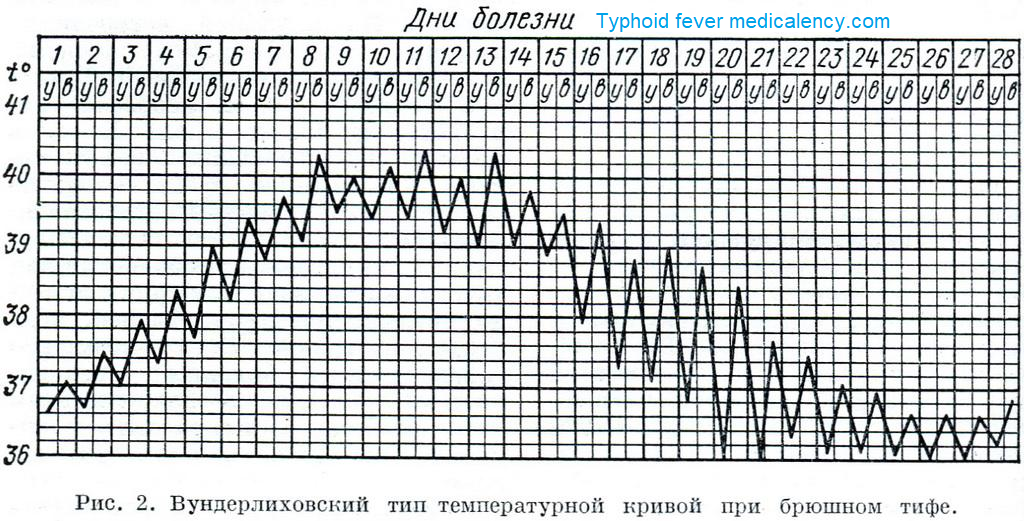
Fig 2 a Russian language example of a typhoid fever “fever curve”
In this particular typhoid patient, the temperature went from 38.7oC to 36oC to 38.5oC on day 19-20. This translates to 101.7oF, 96.8oF 101.3oF. Did this patient experience feeling hot, followed by “the chills” to feeling hot again as some Covid-19 patients report?  It is easier to find “fever curves” for typhoid fever 150 years ago than to find “fever curves” for Covid-19. Covid-19 patients who are not too “out of it” can be turned into citizen scientists by recording their temperatures .
Some undated Wikipedia Commons images for Antipyretic activities
Arsacetin is an arsenic containing compound that was formerly used to treat syphilis and trypanosomiasis.
Fig 3 A fever curve that documents the testing a potential anti-pyretic compound
These patients started out with temperatures of 39.5oC or about 103oF . The patients were given arsacetin Their temperatures dropped to an average of about 36oC or about 96.8oF. These patients had 12 hr stretches in which their temperatures hovered in the low normal range of 36.5oC. We do not know if all 104 cases were given arsacetin at the same time each day. The subsequent daily highs were 37.5oC or about 99.5oF and 37oC or about 98.6oF .
Continuing wih the Wikicommons image search, here we have an old image of a relapsing fever. All we know that there were 30 patients treated with something.
Fig. 4 A fever curve showing gradual reduction of daily high temperatures over the course of several days.
In this case there was a linear decline of peak daily body temperatures of 40oC, 39.5oC, 39oC and 38.5oC. . . .. or about 104 oF, 103oF, 102 oF, and 101oF. If we did not continue to monitor the body temperature of this group for several days, we may easily have concluded that the treatment cured the fever in a few hours. Ironically, some of the anti-pyretic clinical trials on clinicaltrials.gov do not take into account diurnal variations in temperatures.
Absent from the fever curve in figure 4 is the placebo. The savvy reader might ask, “how do we know the the fever wouldn’t just go away as the patients recover from the infection?”  This is something we are doing right in this modern age. A placebo is an inactive substance thought to have no biological activity. If a patient believes that taking some pill is going to cure them, the fever might go away faster because their stress level is reduced.
Diurnal temperature variations and melatonin
This particular temperature curve for a malarial fever seems to track diurnal temperatures. The nice thing about this image is that the physician recorded more than just the high and low temperature of the patient for several days.
Fig. 5 Left, fever curve for malaria. The last 24 hours were retraced in cyan. Right diurnal variations in rectal temperature (cyan) and melatonin (magenta), adapted from reference [2]. 15:00 would be about 3 PM. 19:00 is 7 PM, the sun is starting to set, most of the year. Reference [2] does a really nice job of summarizing the role of light in melatonin secretion and sleep. Note that just because melatonin is going down as body temperature is going up, one is causing the other.
Anderson and Reitner [3] make a strong argument for the role of melatonin and switching immune cells from inefficient glycolytic metabolism to more efficient mitochodrial oxidative phosphorylation. Melatonin induces the circadian gene, Bmal1, which disinhibits the pyruvate dehydrogenase complex (PDC).  PDC drives mitochondrial conversion of pyruvate to acetylâ€coenzyme A (acetylâ€CoA). Acetyl CoA feeds into the tricarboxylic acid cycle that generates reducing equivalents for the electron transport chain. The electron transport chain is the primary souce of ATP in metabolically active cells. Anderson and Reitner [3] discuss the Covid-19 cytokine storm turning off the pineal gland production of melatonin. We seen diurnal temperature variations in two of the three examples of typhoid fever curves [1]. These variations were turned off in the patient that died [1], see Fig 1.
Is melatonin production turned off in severe Covid-19 but not in mild cases? Unfortunately, “fever curves” are not as popular in 2020 as they were in the mid to late 1800s.
Time of day matters in fighting an infection
In bacterial septic shock, temperatures may go above or below average. Circulatory collapse due to hypo-tension is another aspect of this killer. Bacterial lipo polysaccaride (LPS) is what sets things off. Mitochondria are important thermo controllers. Does the time of day that a mouse sees LPS predict it’s outcome. A group of scientists from Aires, Argentina tested this hypothesis [4]. In the experiments conducted under LD conditions, animals were injected with LPS at
ZT11 …. Melatonin has been high for a while.
ZT19…. Melatonin has been low for a while.
(ZT: zeitgeber time; ZT0: time of lights on; ZT12: time of lights off)Â Note that the authors did not mention melatonin in their publication.
Fig 6, adapted from [4] A. survival curve B. temperature after LPS or vehicle injection
After eight days, 80% of the mice injected with LPS as they were settling into sleep (ZT11) were alive. Fig 6A
After eight days, two thirds of the mice injected with LPS in the morning were dead. Fig 6A.
Mice injected with the solvent used to dissolve the LPS maintain a constant body temperature regardless of the time of day of the injection, Fig 6B
TNF-α in serum are higher in those mice inoculated at ZT11 compared to ZT19 (not shown)
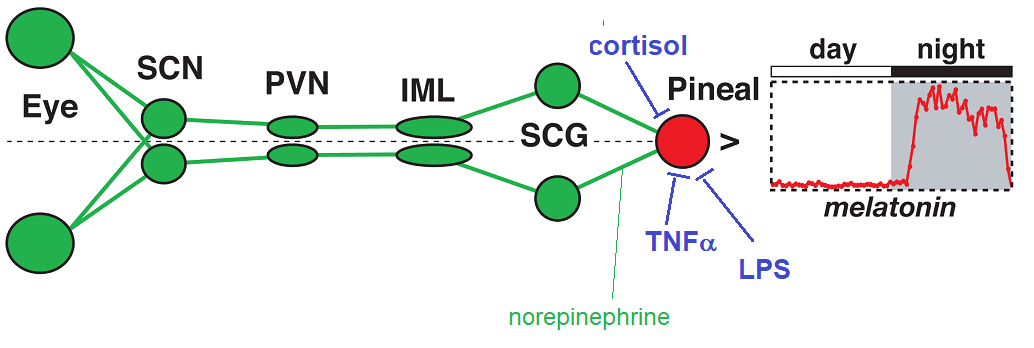
Pineal Gland Pathways
Light entering the eye evokes a signal n the retina that is transmitted to the supra chiasmic nucleus (SCN) to the paraventricular nucleus (PVN), to the
intermediolateral column (IML) and then the cells from the superior cervical ganglion (SCG). These cells secrete norepinepthrin (also noradrenaline). Reference [5] describes how norepinephrine controls the translation of melatonin synthesis gens into proteins. This process may be blocked by agents involved in infections, see figure 7.
Fig7 Pathways from light entering the eyes to synthesis of melatonin. The superior cervical ganglion (SCG) stimulates melatonin production by release of noripinephrine.
The role of the locus ceruleus in temperature control
When we exercise at night or during the day, we experience vasodilation and sweating to cool ourselves down. Machado and coworkers measured rat tail vein vasodilation in response to intense exercise [8]. They found the absolute threshold for vasodilation was higher in the dark-phase: 39.3 ± 0.02°C vs. 38.5 ± 0.02°C in the light-phase. [7]
Fig. 8 Light to the locus ceruleus (LC) norepinephrine system.  The LC/NE has the supra chiasmic nucleus (SCN) in common with the pineal/melatonin system. The Dorsomedial hypothalamic nucleus is different.  The locus secretes norepinephrine to communicate with the Paraventricularis of the Hypothalamus (PVN) and much more.
Fig 8 is a fusion of an image in reference [8] and Fig 7 to make the point that far more goes into controlling body temperature than just melatonin. Chemically destroying the locus ceruleus blunts the fever response to lipopolysaccharide (LPS). [9] Kaneko and coworkers followed up on a previous study that showed an increase in NE in the locus ceruleus of mice injected with LPS at time points of two and four hours. [10] As a followup these authors examined gene expression of TNFα and IL-1β. LPS into the abdominal cavity of rats. [10] TNFα and IL-1β mRNA peaked at 2 and 4 hours then decreased to control levels. [10] TNFα is produced by microglia, not the neurons of the locus ceruleus that secrete NE. Kaneko and coworkers isolated microglia from neonatal mouse brains. Cultured microglia were treated with LPS ± 1 µM NE. NE down regulates TNFα on both the mRNA and protein level.The results point to an anti-inflammatory role of NE.
Conclusions
We’ve know for over 150 years that diurnal temperature variations often persist with infections that cause fevers.
Both the pineal gland (melatonin) and the locus ceruleus (norepinephrine) respond to light/dark cycles via the supra chiasmic nucleus (SCN). We cannot blame a fever getting better or worse at normal diurnal highs on either the pineal gland and/or the locus ceruleus.
LPS, the mediator of bacterial inflammation, interacts with both the pineal gland and the locus ceruleus.
Even after 150 years, it still feels like we know little about the diurnal variation of fevers that are associated with infections.
Bored and quarantined at home with a fever, the citizen scientist can help out by simply recording their oral temperature throughout the day. The more points, the better. Just two points at 6AM and 6 PM is a good start. This post describes how fever curves have been used in clinical trials.
References
Hess V, Berlin C, Mendelsohn JA(2010) Case and Series: Medical Knowledge and Paper Technology, 1600–1900 History of Science [CrossRef]
Lack LC, Wright HR (2007) Chronobiology of sleep in humans. Cell. Mol. Life Sci. 64 1205 – 1215 [Cross Ref]
Anderson G, Reiter RJ. (2020) Melatonin: Roles in influenza, Covid-19, and other viral infections. Rev Med Virol. 30(3):e2109. [PubMed free article]
Markus RP, Fernandes PA, Kinker GS, da Silveira Cruz-Machado S, Mar̤ola M. (2018) Immune-pineal axis Рacute inflammatory responses coordinate melatonin synthesis by pinealocytes and phagocytes. Br J Pharmacol. 175(16):3239-3250.[PMC free article]
Almeida MC, Steiner AA, Coimbra NC, Branco LG(2004)Thermoeffector neuronal pathways in fever: a study in rats showing a new role of the locus coeruleus.J Physiol. 558(Pt 1):283-94. [PMC free article]
Machado FS, Fóscolo DR, Poletini MO, Coimbra CC.(2016) Influence of Time-of-Day on Maximal Exercise Capacity Is Related to Daily Thermal Balance but Not to Induced Neuronal Activity in Rats. Front Physiol. 2016 Oct 14;7:464.[PMC free article]
Atzori M, Cuevas-Olguin R, Esquivel-Rendon E, Garcia-Oscos F, Salgado-Delgado RC, Saderi N, Miranda-Morales M, Treviño M, Pineda JC, Salgado H. (2016) Locus Ceruleus Norepinephrine Release: A Central Regulator of CNS Spatio-Temporal Activation? Front Synaptic Neurosci. 2016 Aug 26;8:25. [Cross Ref]
Almeida MC, Steiner AA, Coimbra NC, Branco LG(2004)Thermoeffector neuronal pathways in fever: a study in rats showing a new role of the locus coeruleus.J Physiol. 558(Pt 1):283-94. [PMC free article]
Kaneko YS, Mori K, Nakashima A, Sawada M, Nagatsu I, Ota A(2005)Peripheral Injection of Lipopolysaccharide Enhances Expression of Inflammatory Cytokines in Murine Locus Coeruleus: Possible Role of Increased Norepinephrine Turnover 94(2):393-404. [Cross Ref]
Fever curves are an interesting source of amusement for those that have the ability to collect the data. This is especially true for those experiencing periodic fever or chills.
Paracetamol, acetominophen, propacetamol are inhibitors of cyclooxygenase (Cox). Some references suggest it might interact with the endocannabinoid system.   Dexibuprofen, like its more structurally heterogenous ibuprofen, is a nonsteroidal anti-inflammatory drug (NSAID). Cox is part of the pathway that converts arachindonic acid (AA) to the pro-inflammatory cytokine PGE2.
Fevers in kids [1]
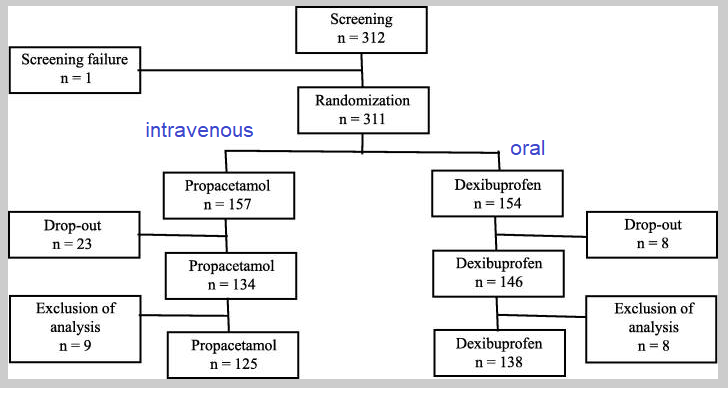
This study looked at fevers that accompany upper respiratory track infections (URTI) in children. The kids were given oral dexibuprofen or intravenous propacetamol. The rationale was that if a kid is vomiting, oral antipyretics are ineffective.  Auxillary (armpit) temperatures were recorded every 30 minutes. This was an Equivalence Trial, a trial with the primary objective of showing that the response to intravenous propacetamol differs from oral Ibuprofen by an amount which is clinically unimportant. This is usually demonstrated by showing that the true treatment difference is likely to lie between a lower and an upper equivalence margin of clinically acceptable differences.
Inclusion criteria
Patients ranging in age from 6 months to 14 years admitted for URTI and presenting with fever (defined as body temperature of the axillar fossa ≥38.0 °C) at the time of admission were included.
URTI was diagnosed based on disease history and physical examination carried out by the attending pediatricians.
Exclusion criteria
Patients were excluded under the following circumstances: the patient had been administered antipyretics within 4 h prior to admission,
a history of febrile crisis within the past 6 months,
the presence of severe hematological abnormality, currently receiving treated for or was treated within the past 6 months for nephrologic, hepatologic, pulmonary, endocrine, hematologic, or cardiologic illnesses, neurologic or central nervous system abnormality,
diabetes currently not under control,
suspected lower respiratory tract infection,
severe hemolytic anemia,
under maintenance therapy for bronchial asthma, asthma, urticarial,
allergic reaction history when using aspirin or NSAIDs, physical or psychological status deemed inappropriate for a clinical trial,
participation in another clinical trial involving other drug(s) within the past 4 weeks, and failure to receive informed consent from the patient or parent.
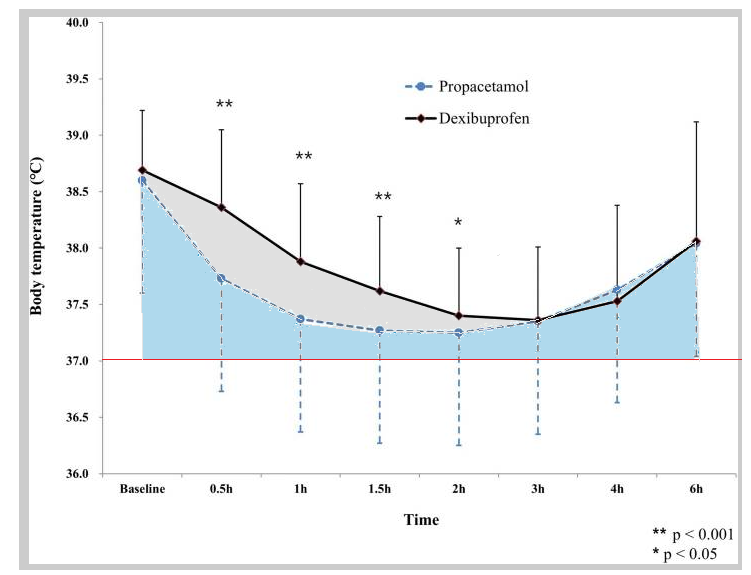
This is what a temperature curve looks like. An attempt has been made to shade the area under the Dexibuprofen curve (gray) versus the Propanecetamol (blue). Notethat the X-axis is time and the Y-axis temperature. The larger the area, the more time the child spends feverish. Some studies on ClinicalTrials.gov like to use  37.0 °C for calculating area under the curve (AUC).
Outcome measurements
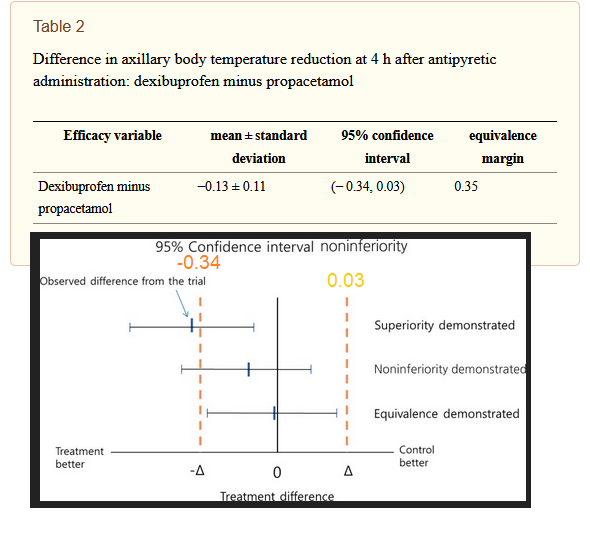
The primary outcome measurement was the difference in body temperature reduction at 4 h after antipyretic administration between the study and control groups.
The authors failed to demonstrate superiority of intravenous propacetamol oral Dexibuprofen.
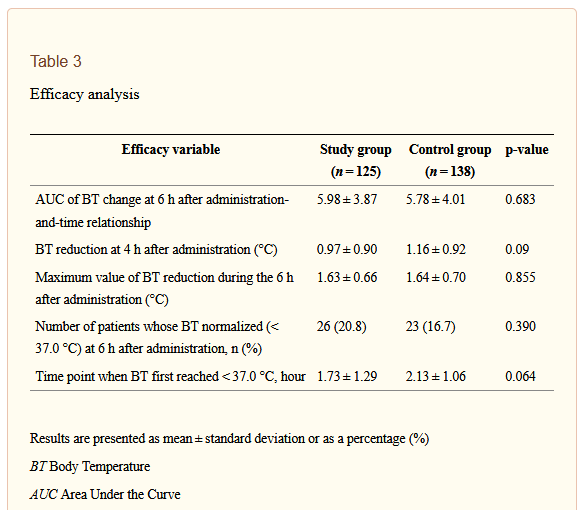
The secondary efficacy variables were range of body temperature reduction at 4 h after antipyretic administration, the Area Under the Curve (AUC) of body temperature change until 6 h after antipyretic administration-and-time relationship,
the maximum value of body temperature reduction within the 6 h after antipyretic administration,
the number of patients whose body temperature normalized (< 37.0 °C) at 6 h after antipyretic administration
the time point when body temperature first reached< 37.0 °C.
Secondary outcome measures are not statistically different
In stroke patients [2]
The investigators compared three common drugs to reduce fevers with no intervention.
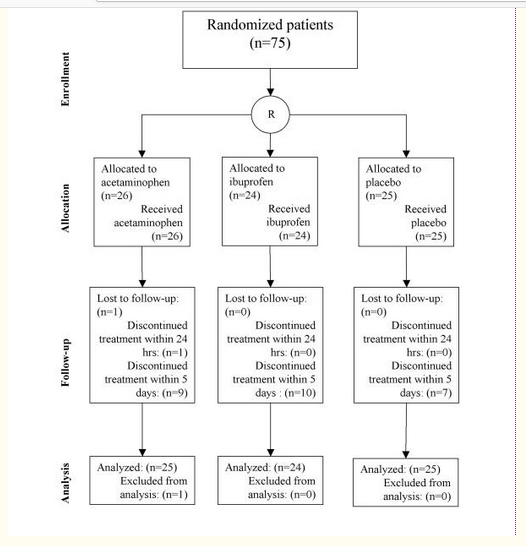
Seventy-five patients with acute ischemic stroke confined to the anterior circulation were randomized to 6 times daily treatments during 5 days after the stroke with either
1000 mg acetaminophen
400 mg ibuprofen
placebo
This study used tympanic temperatures measured every two hours. Treatment was started within 24 hours from the onset of symptoms. Body temperatures were measured at 2-hour intervals during the first 24 hours, and at 6-hour intervals thereafter. We don’t know how diurnal variations in body temperature came into play. We can hypothesize that these patients were not getting a lot of natural sunlight to set their circadian rhythms into motion.
Outcome Measures
Clinical trials have primary and secondary measures to see if the tested intervention has the desired effect on the patient’s outcome.
The primary outcome was body temperature measured rectally at 24 hours from start of treatment. Secondary outcomes were change from baseline temperature at 1 and 5 days from start of treatment, and time with elevated body temperature (> 37.0°C) (area under the curve) during the first 24 hours and the first five days.
Patients could be included if they had
acute ischemic stroke in the anterior circulation
a body temperature between 36.0°C and 39.0°C,
computed tomography (CT) scan that was compatible with acute ischemic stroke
a focal deficit without rapid improvement
and a possibility to start treatment within 24 h after stroke onset.
Exclusion
Patients with a posterior circulation stroke were not included because occasional patients could have severe disturbances of temperature regulation through involvement of the hypothalamus.
Results…
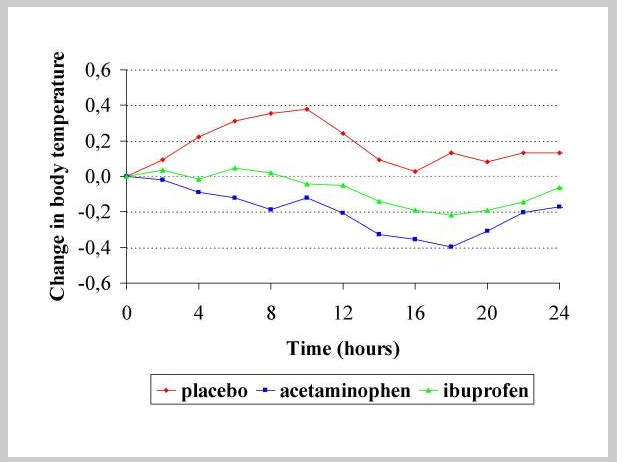
Changes in tympanic temperature after dosing.
Without intervention, the tympanic temperature increases about 0.4 °C in first 8-10 hours after recording, which places us at 8 to 34 hours after the stroke. After about 24 hours the temperature levels off to about 0.2 °C above the starting point.
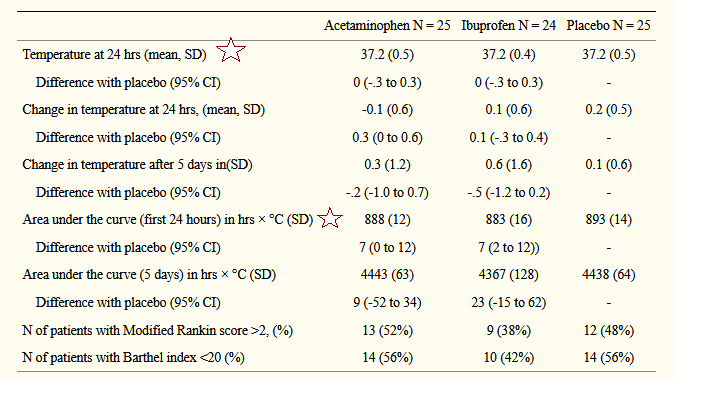
The Barthel Index is a measure of how much a patient needs help with aspects of daily life such as bathing and using the toilet. A score of 20 is functional independence. TheModified Rankin Score is also measures the functional impact of a stroke A score of 2 indicates not back to normal but able to live independently. A score of 5 indicates bedridden.
The antipyretic efficacy and safety of propacetamol compared with dexibuprofen in febrile children: a multicenter, randomized, double-blind, comparative, phase 3 clinical trial
Seung Jun Choi, Sena Moon, Ui Yoon Choi, Yoon Hong Chun, Jung Hyun Lee, Jung Woo Rhim, Jin Lee, Hwang Min Kim, Dae Chul Jeong BMC Pediatr. 2018; 18: 201. [PMC free article]
Dippel, Diederik W J et al. “Effect of paracetamol (acetaminophen) and ibuprofen on body temperature in acute ischemic stroke PISA, a phase II double-blind, randomized, placebo-controlled trial [ISRCTN98608690].†BMC cardiovascular disorders vol. 3 (2003): 2. doi:10.1186/1471-2261-3-2 [PMC free article]
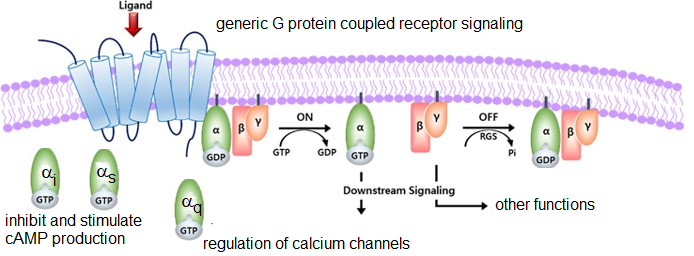
Our featured image is a reminder that the niacin receptor is a member of the G protein coupled receptor family. These receptors talk to each other via α subunits.
Niacin is the other two thirds of Cu(I)NA2., a cuprous niacin supplement available on the market. Most healthcare providers are probably aware of niacin’s many functions.
A big unknown for us is if Cu(I)NA2 can even bind to the niacin receptor. If nothing else, the other two thirds modulate the immune system.
Niacin is a precursor to NAD/NADH2, an H+ / electron carrier in numerous biochemical reactions.
Niacin in high doses causes dilation of the skin’s vasculature in a response called “flush.”
High doses of niacin are available in prescription form as Niaspan® and its generic equivalent “niacin ER” to lower low density lipoprotein (LDL) cholesterol
Niacin receptors in neutrophils and more
Apart from being a precursor of NADH2, niacin has direct physiological actions on its high and low affinity receptors
NIACR1 is also known as the hydroxy carboxylic acid receptor (HCA2) GPR109A, HM74a, HM74b.NIACR2.
NIACR2 is also known as HCA3 and GPR109B. It is the low affinity receptor that is activated by amounts of niacin not normally found in the diet.
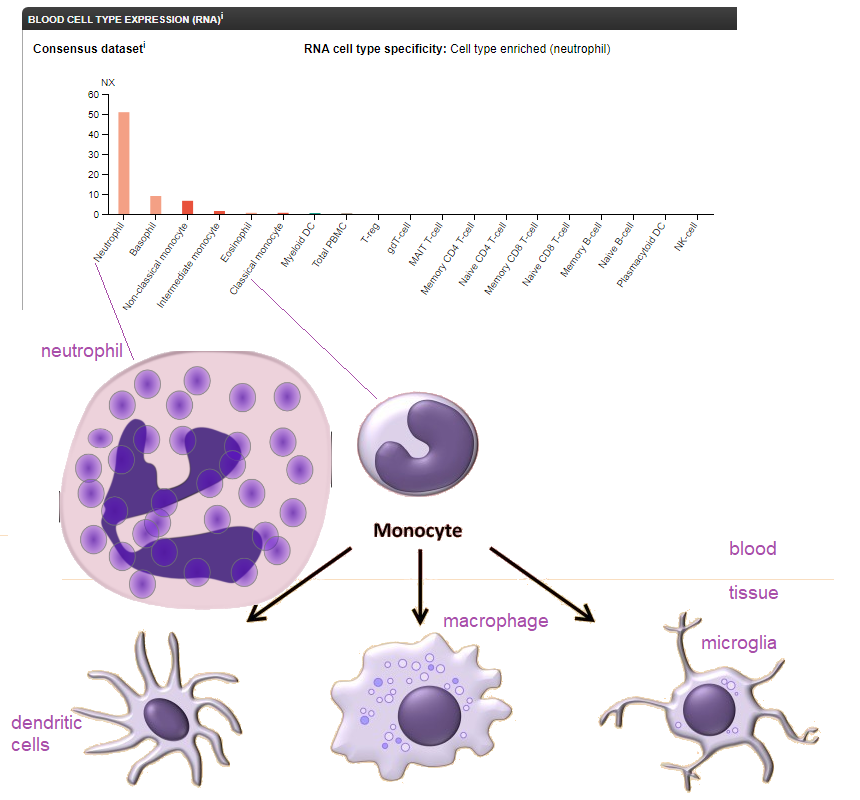
Protein Atlas has compiled some nice data on the mRNA expression of GPR109A in blood cells.
Top. Consensus mRNA expression of GPR109A, a niacin receptor, in blood cells. Bottom Data for dendritic cells, microglia, and macrophage are harder to obtain when they migrate into the tissue site of an infection. GPR109A expression in macrophage may be induced by lipopolysaccharide (LPS) from Gram negative bacteria.
Niacin receptors and cAMP
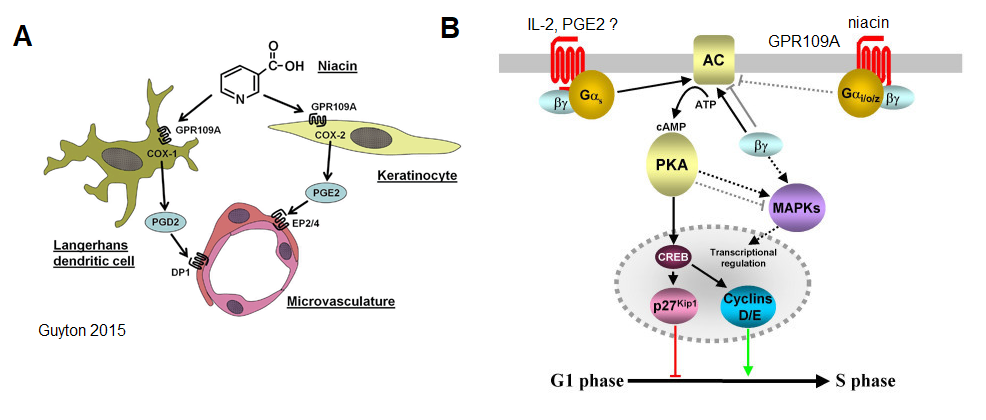
A 2008 study of Kostylina demonstrated that niacin promotes apoptosis, programmed cell death, in mature but not immature neutrophils. This action is mediated by the GPR109A G-protein coupled receptor. G-protein coupled receptors may stimulate or inhibit the enzyme adenylyl cyclase. AC converts cellular ATP to the second messenger cyclic AMP (cAMP). Note the cyan colored βγ subunit. These will come into the discussion of potential niacin signalling in macrophage.
A Niacin GPR109A pathways to vasodilation seen in “flush” B G-protein coupled receptors responsible for pro-survival pathways in neutrophils couple to Gs that activates adenylyl cyclase. The niacin receptor GPR109A couples with Gi that inhibits adenylyl cyclase (AC).
G protein coupled receptor cross talk
The authors did not discuss which G-protein coupled receptor on neutrophils might be simulating adenylyl cyclase by way of a Gs subunit. The interleukin-2 and PGE2 receptors are G-protein coupled receptors that may stimulate neutrophils.
Niacin, GPR109A, and macrophages
Inflammatory mediators LPS ( Gram negative bacteria), zymosan (polysaccharide in yeast, fungi), lipoteichoic acid (LTA, Gram positive bacteria), polyinosine-polycytidylic acid (poly I:C, viruses) induce GRP109A in cultured marcrophage. (Feingold 2014). LPS was able to increase GPR109A mRNA up to 80x in less than 24 hours. Niacin binding to GRP109A receptor may be a means of turning off the initial, innate immune response to pathogens.
Niacin inhibits macrophages by decreasing cAMP
Zandi-Nejad and coworkers (2013) examined the role of niacin on macrophage function. Their primary focus was the role of macrophage in atherosclerosis rather than infectious diseases. The”cytokine storm“, also known as cytokine release syndrome, has gained a lot of attention as a morbidity factor in COVID-19.
Phagocytosis and chemotaxis of blood wild type HCAR2+/+ and HCAR2-/- knock out mouse bone marrow derived marcophage (BBM) was shown to be decreased by nicotinic acid. The HCAR2 gene codes for the GRP9A protein.
HCAR2+/+ and HCAR2-/- BBM. Niacin lowered mRNA transcripts of all of these cytokines after 48 hours of exposure to LPS in the wild type but not in the BBM lacking the GPR109A receptors.
Zandi-Nejad and coworkers (2013) remarked that their results differed from those of Rossi (1998) in that cAMP increases inhibited macrophage. Shi (2017) suggested that niacin macrophage inhibition had more to do with the βγ subunit of heterotrimeric G proteins acting on protein kinase C.
A look back, cAMP and macrophage activity
Rossi (1998) demonstrated that intracellular cAMP decreased the ability of preipheral blood monocyte derived macrophage to phagocytize apoptotic neutrophils but not opsonized red blood cells. These authors also found that PGE2 to be a strong inducer of cAMP.
A look ahead at recent publications
Negreiros-Lima and coworkers (2020) have pushed the boundaries of earlier studies. These authors used a non-hydrolyzable analog of cAMP, db-cAMP to activate protein kinase A pathways. They addressed ways that cAMP modulates the M1 (pro inflammatory) to M2 (anti-inflammatory) transition. To make matters more complicated, they introduced the M2 subsets: M2a, M2b and M2c. We have no idea if the GRP109A receptor is expressed in all of these developmental stages. An additional new term is “effectocytosis” the clearance of neutrophils undergoing apoptosis.
References
Bühler S, Frahm J, Liermann W, Tienken R, Kersten S, Meyer U, Huber K, Dänicke S.(2018) Effects of energy supply and nicotinic acid supplementation on phagocytosis and ROS production of blood immune cells of periparturient primi- and pluriparous dairy cows. Res Vet Sci.116:62-71
Guyton J., Campbell K., Lakey W. (2015) Niacin: Risk Benefits and Role in Treating Dyslipidemias. In: Garg A. (eds) Dyslipidemias. Contemporary Endocrinology. Humana Press, Totowa, NJ
Feingold KR, Moser A, Shigenaga JK, Grunfeld C.(2014) Inflammation stimulates niacin receptor (GPR109A/HCA2) expression in adipose tissue and macrophages. J Lipid Res. 2014 Dec;55(12):2501-8. Link
Kostylina G, Simon D, Fey MF, Yousefi S, Simon HU.(2008) Neutrophil apoptosis mediated by nicotinic acid receptors (GPR109A). Cell Death Differ.15(1):134-42 Link
Negreiros-Lima GL, Lima KM, Moreira IZ, Jardim BLO, Vago JP, Galvão I, Teixeira LCR, Pinho V, Teixeira MM, Sugimoto MA, Sousa LP. (2020) Cyclic AMP Regulates Key Features of Macrophages via PKA: Recruitment, Reprogramming and Efferocytosis. Cells. 9(1). pii: E128. Link
Rossi AG, McCutcheon JC, Roy N, Chilvers ER, Haslett C, Dransfield I. (1998) Regulation of macrophage phagocytosis of apoptotic cells by cAMP. J Immunol. 160(7):3562-8.Link
Shi Y, Lai X, Ye L, Chen K, Cao Z, Gong W, Jin L, Wang C, Liu M, Liao Y, Wang JM, Zhou N. (2017) Activated niacin receptor HCA2 inhibits chemoattractant-mediated macrophage migration via Gβγ/PKC/ERK1/2 pathway and heterologous receptor desensitization. Sci Rep. 2017 Feb 10;7:42279 Link
Zandi-Nejad K, Takakura A, Jurewicz M, Chandraker AK, Offermanns S, Mount D, Abdi R (2013) The role of HCA2 (GPR109A) in regulating macrophage function. FASEB J. 27(11):4366-74. Link
 Medical foods do not require a prescription and are not regulated as drugs. They may provide nutrition when the patient is too incapacitated to get said nutrition from a normal diet. In this case we have a sick guy who just doesn’t feel like eating copper rich foods like liver and kale. In this post we will cover how copper may play a role in the renin angiotensin system (RAS) that may be compromised in severe Covid-19 and other infections.Â
What is the Renin Angiotensin System (RAS)?
Qin and coworkers (2020) first noted hypertension as a risk factor for severe versus mild forms of COVID-19. Lippi and coauthors (March 31, 2020) summarized literature of numerous studies and found a consistent correlation between severe COVID-19 and hypertension. Which came first? Hypertension or Severe Covid-19? Was hypertension pre-existing or the result of the infection? Was pre-existing hypertension controlled by the use of an ACE inhibitor that might have increased the expression of the ACE2 enzyme/COVID-19 receptor? Or was pre-existing hypertension controlled by use of β-adrenergic receptor blockers, controlled by life style changes like low sodium diets, or left uncontrolled?Hao Cheng and colleagues of the Peking University First Hospital of Beijing reviewed risk factors or severe COVID-19 infections and the COVID-19 receptor angiotensin converting enzyme 2 (ACE2). ACE2 is a receptor for other corona viruses. Let us take a closer look at the RAS.
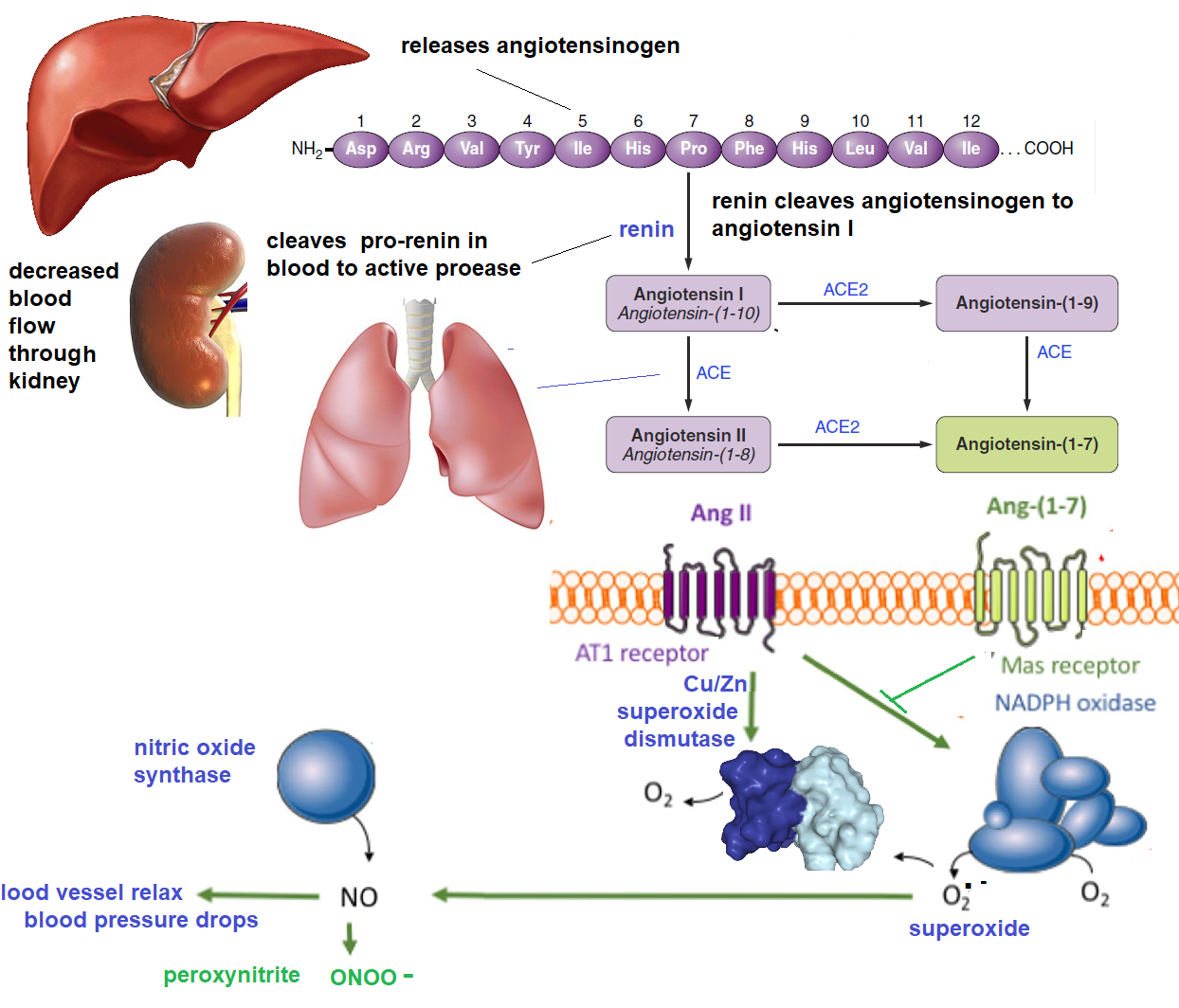
The angiotensin II converting enzyme 2 (ACE2) role in the renin-angiotensin-system (RAS). Cu/Zn superoxide dismutase (SOD) is a brake in the RAS.
 When blood flow to the kidney is decreased, plasma pro-renin is cleaved to the active protease renin. Renin cleaves angiotensinogen to angtiotensin I. Angiotensin converting enzyme (ACE) cleaves angiotensin I to angiotensin II. Angiotensin II binds to the angiotensin receptor 1 (AT1). The primary result is increased expression of NADPH oxidase, a super oxide generating enzyme. Superoxide reacts with with the vasodilator nitric oxide (NO) to produce peroxynitrite. Blood vessels constrict and renal blood flow is increased.
Cu/Zn SOD3 and RAS, a closer look
ACE2, aka the Covid-19 receptor, used to be primarily regarded as the first brake to the RAS. Ozumi (2012) discovered a second brake: increased expression of Cu/Zn superoxide dismuase 3 (SOD3). Activation of the AT1 receptor might even stimulate Cu(I) uptake by the copper transporter Ctr1. Cu(I) is handed off to the Cu(I) chaperone Atox1, a transcription factor for the SOD3 gene.Â
Copper in the +1 oxidation is involved in several levels in producing Cu/Zn SOD3 (1) as acquired by Cu(I) channel Ctr1 (2 ) in chaperone/transcription factor Atox1, (4) in channel ATP7A that loads Cu in Golgi where SOD3 is being processed for secretion.
Multiple levels of regulation…
Sean Didion (2012) chose not to follow up on the Ozumi (2012) suggestion that ATR1 modulates the Ctr1 channel. Didion focused on demonstrating that angiotensin II also increases protein levels of Atox1 and SOD3.
Meanwhile, Wang (2016) reported that SOD3 levels are decreased in the brains of ACE2 knock out mice. If anything, angiotensin II should increase SOD3 in these mice. It should be noted that both the MAS and AT1 receptors signal via heterotrimeric G-proteins.
Abouhashem (May 2020) isolated single cell RNA from alveolar type II epithelial cells. These cells came from elderly and young donors. The mRNA were sequenced and expression levels compared.  The rationale was taht colocalization of ACE2 and TMPRSS2 enables Covid-19 to invade cells. Expression levels of these genes in the alveolar type II cells of elderly and young patients were comparable. In cells from the elderly, 263 genes were down regulated and 95 up regulated.  Superoxide dismutase 3 (SOD3) was identified as the top-ranked gene that was most down regulated in the elderly. The authors proposed that SOD3 and the ATF4 transcription factor -related antioxidants will work in synergy with promising antiviral drugs such as remdesivir to further improve COVID-19 outcomes in the elderly.
Cheng (2020) discussed ACE2 as one means of applying the brake to the RAS increase in blood pressure. COVID-19 binding to ACE2 might compromise this brake. There is an internal feedback loop that involves Cu(I). One way or another, SOD3 expression is increased by angiotensin 1-7 and aginiotensin II (aka 1-8). A functional SOD3 enzyme requires repletion with copper in the +1 oxidation state.
In summary
To the invited guest reading this post, we are not making claims at this point. We do want to remind you that the copper binding protein Atox1 regulates the expression of SOD3. We do not know if these elderly volunteers were copper deficient compared to younger volunteers.
RAS, not just corona virus infections
The COVID-19 infection is just one example in which the RAS system might be activated: (1) decreased fluid intake due to compromised GI function that is not quite diarrhea and (2) direct activity of the virus on the RAS. Naturally healthcare professionals would be involved in assays involved with plasma SOD3 activity and copper content of ceruloplasmin.
But also bacterial infections
Bacterial sepsis involves SOD3. Constantino (2014) induced bacterial sepsis in a rat cecal ligation and preforation model. Cecal perforation would be akin to an appendicitis in humans. These authors found an increase in SOD3 levels following sepsis that were not able to totally prevent oxidative stress and inflammation associated with ONOO− production. While the rats should not have been copper deficient, the role of supplemental to replete the new production of SOD3 was not examined. Mechanism(s) of increased SOD3 were not examined, but one would expect activation of the RAS in response to the massive vascular collapse that is associated with sepsis. Human patients experiencing an appendicitis would not be boosting their serum copper via normal Cu(I) found in foods. Cu(I)NA2 administered as a medical food would have to be done under the supervision of a physician.
And also yeast infections
Candida (yeast ) infections offer another twist to SOD3 and Cu(I). Yeast express a zinc free, Cu only, superoxide dismuase (SOD5) that enables them to survive super oxide produced in the phagosomes of macrophage and neutrophils. SOD5 is an extracellular enzymes attached to the cell membrane by way of glyosylphosphatidylinositol linkages (Gleson 3015).
Unlike mammalian secreted SOD3, SOD5 does not use these Golgi proteins
the copper chaperone Atox1
copper-transporting ATPases
Gleason (2014) also proved that, unlike intracellular mammalian SOD1, yeast SOD5 does not require
a CCS chaperone
Yeast acquires Cu(II) from the extracellular mileau of the host.
This host source might be Cu(II) bound to albumin. Robinette (2020) compared the affinities yeast copper only SOD5 and bovine SOD1 for copper using Cu(II) chelators. They found that SOD1 has a higher affinity for Cu(II) than yeast SOD5. The right Cu(I) copper supplement may
feed the patient’s SOD3 and SOD1
while not feeding Cu(II) to SOD5 of the yeast pathogen.
If one cannot absorb copper from food because of an illness
. It is proposed that Cu(I)NA2 is a way of obtaining copper in its +1 oxidation state for those who are too sick to eat the large amounts of copper rich foods to get said copper in its natural +1 oxidation state. Any infection, be it fungal, viral, or bacterial is associated with large production of the reactive oxygen species super oxide.Â
Septic shock is also associated with vascular collapse and the associated activation of the Renin-Angiosystem-System. Angiotnsin II has even been explored as a means of preventing vascular collapse and multi-organ failure (Corrêa 2015).Â
As reviewed in this post, angiotensin II is also a way of boosting blood levels of Cu/Zn SOD3. Â
No appetite or unable to eat copper containing foods
While Cu(I)NA2 has the same oxidation state as copper naturally occurring in the food we eat, it is a processed product to deliver required amounts of copper to patients who are too ill to large amounts of food. In the case of infections it is critical that enzymes such as superoxide dismutase are replete with the copper cofactor.
Feeling too sick to eat is a common symptom of many illnesses, not just infections. COVID-19’s affect on the GI tract may be under recognized according to a letter by Weicheng Liang and colleagues to the British Medical Journal Gut. These authors argued that while only a smaller fraction of COVID-19 patients had out right diarrhea, the small intestine might be compromised and the sight of COVID-19 infection due to the extensive GI expression of ACE2, the receptor for the COVID-19 spike glycoprotein.
Unable to eat
The appendicitis patient may be NPO, “nil per os”…. “nothing by mouth.”  A few arguments for non oral routes for drug status…
No duodenum…Â Griffith (2009) was one of the first to report copper deficiency secondary to the “roux-en-Y” gastric bypass that may takes the duodenum and 100-300 cm of the proximal jejunum. This is one of many papers addressing this particular problem.
Absorption by the colon Charlie Barker, owner and CEO of Mitosynergy, has talked of colonic andministration of Cu(I)NA2 via the rectal route. My big questions for gatroenterlogists would (1) Are appendicitis patients NPO because Vagas nerve stimulation make the condition worse? (2) Does injecting something into the patient’s colon via the rectum stimulate the Vagus nerve?
 Cu+ transporters in the colon Here is an overview of the Cu(I) transporter Ctr1 offered by ProteinAtlas.org. It become readily apparent from the brown antibody staining why gastric bypass patients may become copper deficient.
Antibody staining against the Ctr1 Cu(I) transport protein failed to demonstrate expression in the oral mucosa and salivary gland. A small amount of expression was found in the esophagus and colon. Moderate expression was found in the duodenum. Nuclei are stained blue. Ctr1 stains brown.
Cu(I)NA2Â already has clearance from the FDA as a new dietary ingredient. In an infection such as COVID-19 that can compromise the gastrointestinal tract, obtaining the proper dose may require medical supervision. This supervision may include
rectal administration bypassing the oral route
measuring the superoxide dismutase level in the patient’s blood
or the copper load in the Cu(I) carrier protein ceruloplasmin.
Abouhashem AS, Singh K, Azzazy HME, Sen CK. (2020) Is Low Alveolar Type II Cell SOD3 in the Lungs of Elderly Linked to the Observed Severity of COVID-19? Antioxid Redox Signal. 2020;10.1089/ars.2020.8111. Link
Cheng H, Wang Y, Wang GQ. (2020) Organ-protective Effect of Angiotensin-converting Enzyme 2 and its Effect on the Prognosis of COVID-19. J Med Virol. 2020 Mar 27. Review. Link
Constantino L, Gonçalves RC, Giombelli VR, Tomasi CD, Vuolo F, Kist LW, de Oliveira GM, Pasquali MA, Bogo MR, Mauad T, Horn A Jr, Melo KV, Fernandes C, Moreira JC, Ritter C, Dal-Pizzol F. (2014) Regulation of lung oxidative damage by endogenous superoxide dismutase in sepsis. Intensive Care Med Exp. 2014 Dec;2(1):17. Link
Corrêa TD, Takala J, Jakob SM.(2015)Angiotensin II in septic shock. Crit Care. 2015 Mar 16;19:98 Link
Didion SP.(2012) Antioxidant 1 in hypertension: more than just a copper chaperone. Hypertension. 60(2):285-7 Link
Gleason JE, Galaleldeen A, Peterson RL, Taylor AB, Holloway SP, Waninger-Saroni J, Cormack BP, Cabelli DE, Hart PJ, Culotta VC. (2014) Candida albicans SOD5 represents the prototype of an unprecedented class of Cu-only superoxide dismutases required for pathogen defense Proc Natl Acad Sci U S A. 111(16):5866-71. Link
Griffith DP, Liff DA, Ziegler TR, Esper GJ, Winton EF.(2009) Acquired copper deficiency: a potentially serious and preventable complication following gastric bypass surgery. Obesity (Silver Spring).17(4):827-31. Link
Liang W, Feng Z, Rao S, Xiao C, Xue X, Lin Z, Zhang Q, Qi W. (2020) Diarrhoea may be underestimated: a missing link in 2019 novel coronavirus. Gut. 2020 Feb 26. pii: gutjnl-2020-320832. Link
Lippi G, Wong J, Henry BM.(2020) Hypertension and its severity or mortality in Coronavirus Disease 2019 (COVID-19): a pooled analysis. Pol Arch Intern Med. 2020 Mar 31. Link
Meng J, Xiao G, Zhang J, He X, Ou M, Bi J, Yang R, Di W, Wang Z, Li Z, Gao H, Liu L, Zhang G. (2020)Renin-angiotensin system inhibitors improve the clinical outcomes of COVID-19 patients with hypertension. Emerg Microbes Infect. 9(1):757-760. Link
Ozumi K, Sudhahar V, Kim HW, Chen GF, Kohno T, Finney L, Vogt S, McKinney RD, Ushio-Fukai M, Fukai T. (2012) Role of copper transport protein antioxidant 1 in angiotensin II-induced hypertension: a key regulator of extracellular superoxide dismutase.Hypertension. 60(2):476-86. Link
Qin C, Zhou L, Hu Z, Zhang S, Yang S, Tao Y, Xie C, Ma K, Shang K, Wang W, Tian DS. (2020) Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clin Infect Dis. 2020 Mar 12. pii: ciaa248.
Robinett NG, Culbertson EM, Peterson RL, Sanchez H, Andes DR, Nett JE, Culotta VC. (2019) Exploiting the vulnerable active site of a copper-only superoxide dismutase to disrupt fungal pathogenesis. J Biol Chem. 294(8):2700-2713 Link
Wang XL, Iwanami J, Min LJ, Tsukuda K, Nakaoka H, Bai HY, Shan BS, Kan-No H, Kukida M, Chisaka T, Yamauchi T, Higaki A, Mogi M, Horiuchi M. (2016) Deficiency of angiotensin-converting enzyme 2 causes deterioration of cognitive function. NPJ Aging Mech Dis. 2016 Oct 20;2:16024. Link
These are some thoughts addressing whether Cu(I)NA2  could be used as a medical food to treat various infections in addition to COVID-19 that is making the news as of this posting.  This “proper copper thought was inspired by the study of Qin (2020) study that showed an increase in the neutrophil to lymphocyte ratio in severe cases of COVID-19.  Early studies of Cu(I)NA2 show that it decreases neutrophils and increases lymphocytes in humans and fish. The ratio of neutrophils to lymphocytes has gained popularity as a prognostic marker in infectious diseases.  Don’t we need both? The following is a Devil’s Advocate examination of copper and its deficiency in sepsis. Your comments are invited.
While the pandemic is over, we still have SARS-Cov2 and plenty of other infections.
Does the neutrophil to lymphocyte ratio matter?
Dr Lagunas-Ramal (2020) has called for use of the neutrophil to lymphocyte ratio as a metric.  of hyper-inflammation to predict which cases of COVID-19 are likely to progress to becoming severe. Most hospitals in places like Mexico have the instrumentation to perform such tests. Cu(I)NA2 has been shown to decrease neutrophils and increase lymphocytes in a human clinical trial and in two fish studies. Neutrophils are not only the first line of defense of the innate immune system but also a source of reactive oxygen species (Kircher 2012).
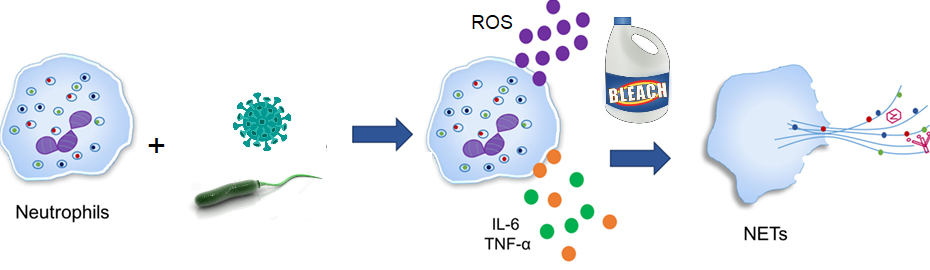
A diagram of hematopoietic cell lineage. Myeloid progenitors give rise to the cell of the innate immune system whereas lymphoid progenitors give rise to cells of the antibody producing acquired immune systems. Monocytes differentiate into antigen presenting dendritic cells and macrophage that present antigen to T cells. Neutrophils release the neutrophil extracellular trap: a combination of DNA, histones, and enzymes.
Neutrophils have gotten a bad reputation in the prognostic value of the neutrophil to lymphocyte ratio. Kirchner and coworkers (2012) demonstrated that NADPH oxidase generated superoxide and myeloperoxidase generated hypochlous (bleach) are involved in production of the neutrophil extracellular trap (NET). Myeloperoxidase produces hypochlorous acid from the Cl– anion and hydrogen peroxided, H2O2. NET is composed of DNA and a variety of antimicrobial proteins.
As of 15 April 2020 (Velavan review) low lymphocyte counts were still considered to be a predictor of severe COVID-19 cases. T- and B-cell differentiation factor interleukin 6 (IL-6), C-reactive protein (CRP), and fimbrin degradation product D-dimer were added to the list of predictors of severe COVID-19.
Do NETs catch viruses?
Do NETs catch viruses? We do not currently have information on the Corona virus family but have the influenza study of Tang (2019).
These authors started with 720 patients who met the World Health Organization’s criteria for influenza. Influenza cases were confirmed with PCR. Messenger RNA was extracted from whole blood from confirmed cases in order to determine which mRNA best differentiate severe cases that require a ventilator versus those that do not. Healthy controls were also added to the analysis.
Each mRNA message was identified and quantitated with microarray analysis.
Messages were grouped according to protein function in the disease process.
Of the six modules with predictive power, the “neutrophil module†had the best ability to differentiate severe from moderate cases of influenza.
The NET protein myeloperoxidase was one of the top proteins expressed more in severe cases of influenza compared to mild cases.
Ni and coworkers (2019) found that septic patients admitted to the hospital with a high neutrophil to lymphocyte ratio were less likely to die in the hospital. Similar use of the NLR has yet to take hold in the literature as a prognostic test for yeast pathogens like Candida species. A recent review (Patricio 2019) has compared differences in the immune response to Candida which may involve
outer layer of mannose rich N-linked glyco proteins
an inner layer of chitin
activation of host NADPH oxidase, an iron containing generator of superoxide
activation of NET along with enzymes that attack the fungal pathogen
The Patricio review (2019) goes into great detail of the ways in which the innate immune and adaptive immune systems communicate with one another by way of cytokines. These authors argue that if the balance shifts to the innate immune system, persistent inflammation-immune suppression, catabolism syndrome (PICS) can occur. Compensatory anti-inflammatory response syndrome (CARS) occurs when anti-inflammatory cytokines, some of which are secreted by T and B lymphocytes, turn off the immune reaction prematurely. These authors suggested the value of prognostic tests. We need innate and adaptive arms our immune systems. From early studies we know that neutrophils need copper. These early studies supplied copper in the Cu(II) oxidation state. We are proposing that copper in the Cu(I) oxidation state may bring better balance.
and COVID-19 in particular?
A review published in April of 2020 (Barnes) reported finding evidence of NET deposits in a lung biopsy of a deceased COVID-19 patient. This prompted the authors to review the literature. The authors made some interesting points.
Histones in NET also bind to phospholipids in platelets triggering the clotting cascade by activating platelets. This might explain blot clots and strokes seen in younger COVID-19 patients.
Barnes (2020) proposed a loop that involves NET ⇒ IL1β⇒accelerated
Barnes (2020) made brief mention of neutrophil elastase, a protease that degrades the extracellular matrix.  This damage may be repaired by lysyl oxidase (LOX),a copper containing amine oxidase that cross links extracellular matrix proteins elastin and collagen.
Another very recent study from Yu Zuo and collaborators (2020) found myeloperoxidase-DNA complexes and citrinullated histones in the sera of COVID-19 patients.  NETs were found to be associated with COVID-19 cases requiring mechanical ventilation. Further correlation was found with NET components cell-free DNA- myeloperoxidase.  COVID-19 sera trigger control neutrophils to release NETs.
Early Studies: Neutrophil and Macrophage activity in Cu deficiency
Jones and Suttle (1981) compared the ability of leukocytes ( presumably macrophage and neutrophils) from copper deficient (< 8 µM in plasma ) and copper sufficient (> 8 µM in plasma ) ewes and lambs to kill the yeast pathogen Candida albicans. Copper deficiency in ewes and lambs decreased the candidacidal activity in ewes and lambs. Copper deficiency further resulted in a decrease in superoxide dismuase activity in erythrocytes and leukocytes.
Babu and Failla (1990) studied the affect of dietary copper on macrophage and neutrophil activity in weaned male rats for a period of five weeks.
adequate (7 mg/kg diet; +Cu)
deficient (0.7 mg/kg diet; -Cu)
The following were found to decrease as a result of five week copper deficiency
Cellular Cu concentration
activity of Cu,Zn superoxide dismutase (Cu,Zn-SOD),
neutrophil generation of superoxide anion (O2–) in response to opsonized zymosan, phorbol myristate acetate
candidacidal activity
While phagocytic activity was independent of copper, survival of Candida albicans injected into the peritoneal cavity was greater in Cu-deficient rats than in controls. The authors tested a gradient of dietary copper to differentiate between the double edge sword of superoxide to kill the yeast and SOD to prevent the super oxide from killing the rat host. Candidacidal activity were significantly lower in neutrophils from rats fed diets with less than or equal to 2.7 mg Cu/kg feed compared to control cells. Reduced erythrocyte Cu,Zn-SOD activity was observed only when dietary Cu was less than or equal to 2.0 mg/kg feed. A follow up study (Balla 1994) noted an increase in T cell proliferation in male mice on copper sufficient versus copper deficient diets in response to a mitogen that seems to operate via an Interleukin pathway.
Of the Cu carrier protein and neutrophils
and coworkers were interested in the role of Cu(I) bound ceruloplasmin protects neutrophils from apoptosis, programmed cell death, as a means of ending the acute phase of a neturophil mediated immune reaction. Several lines of evidence led them to this interest
Ceruloplasmin (CP) is a Cu and Fe carrier protein P is a ferro:O2-oxidoreductase.
CP is found in the blood plasma as well as interstitial fluid.
CP concentration increases 4x in response to inflammation.
CP is an anionic protein that interacts with and inhibits cationic proteins of the NET such as lactoferrin and myeloperoxidase.
The authors were primarily interested in an in vitro model of chronic inflammation induced by the cytokine TNF-α . They compared Cu replete with holo CP as well as some proteolytic fragments. The Cu replete versus apo (copper deficient) are the most relevant for Cu(I)NA2 as a medical food for sepsis.
Some findings of this study are
Cu CP, but not apo CP, reduced intracellular super oxide generation by neutrophils.
This was observed n the presence and absence of TNFα.
Intracellular reactive species, that include H2O2, were increased by Cu(I) CP but not by apo CP.
Intact, Cu CP promoted neutrophil survival.
The observation that superoxide decreased and H2O2 increased suggested that intracellular Cu/Zn SOD1 might have been Cu deficient.
And there are more Cu-ceruloplasmin interactions…
Kostevich (2015) demonstrated that Cu is necessary for CP binding to macrophage migration inhibitory factor (MIF). MIF is considered pro-inflammatory. Increased MIF levels are correlated with low survival in sepsis patients. This is not the end of the list. If Cu(I)NA2 is to be used as a medical food in patients with sepsis, perhaps a good index of dosing would be measuring Cu content of ceruloplasmin in the patients serum. Neutropils are good first responders. They just need to be kept in check with copper containing enzymes so that second ponderers can take over.
References
Babu U, Failla ML. Respiratory burst and candidacidal activity of peritoneal macrophages are impaired in copper-deficient rats. J Nutr. (1990) 120:1692–9. 10.1093/jn/120.12.1692
Babu U, Failla ML. (1990) Copper status and function of neutrophils are reversibly depressed in marginally and severely copper-deficient rats. J Nutr. 120:1700–9. 10.1093/jn/120.12.1700
Bala S, Failla ML, Lunney J. (1990) Alterations in Splenic Lymphoid Cell Subsets and Activation Antigens in Copper-Deficient Rats. Ann N Y Acad Sci 1990;587:283–5. Link
Barnes BJ, Adrover JM, Baxter-Stoltzfus A, Borczuk A, Cools-Lartigue J, Crawford JM, Daßler-Plenker J, Guerci P, Huynh C, Knight JS, Loda M, Looney MR, McAllister F, Rayes R, Renaud S, Rousseau S, Salvatore S, Schwartz RE, Spicer JD, Yost CC, Weber A, Zuo Y, Egeblad M. (2020) Targeting potential drivers of COVID-19: Neutrophil extracellular traps.J Exp Med. 2020 Jun 1;217(6). pii: e20200652 Link
Cintia PG, Leonardo M, Israel OR, Andrea S, Beatriz VL, Elena DM.(2016) Superoxide Dismutase Activity, Hydrogen Peroxide Steady-State Concentration, and Bactericidal and Phagocytic Activities Against Moraxella bovis, in Neutrophils Isolated from Copper-Deficient Bovines. Biol Trace Elem Res. 171(1):94-100.
Golenkina EA, Viryasova GM, Galkina SI, Gaponova TV, Sud’ina GF, Sokolov AV. (2018) Fine Regulation of Neutrophil Oxidative Status and Apoptosis by Ceruloplasmin and Its Derivatives. Cells. 2018 Jan 12;7(1). pii: E8Â Link
Jones DG, Suttle NF.(1981) Some effects of copper deficiency on leucocyte function in sheep and cattle. Res Vet Sci.31(2):151-6.
Kamiya T, Takeuchi K, Fukudome S, Hara H, Adachi T. (2018) Copper chaperone antioxidant-1, Atox-1, is involved in the induction of SOD3 in THP-1 cells. Biometals.31(1):61-68.
Kirchner T, Möller S, Klinger M, Solbach W, Laskay T, Behnen M. (2012) The impact of various reactive oxygen species on the formation of neutrophil extracellular traps. Mediators Inflamm. 2012;2012:849136
Kostevich VA, Sokolov AV, Grudinina NA, Zakharova ET, Samygina VR, Vasilyev VB.(2015)Interaction of macrophage migration inhibitory factor with ceruloplasmin: role of labile copper ions. Biometals. 28(5):817-26
Lagunas-Rangel FA. (2020) Neutrophil-to-Lymphocyte ratio and Lymphocyte-to-C-reactive protein ratio in patients with severe coronavirus disease 2019 (COVID-19): A meta-analysis J Med Virol. 2020 Apr 3. doi: 10.1002/jmv.25819. [Epub ahead of print]
Ni J, Wang H, Li Y, Shu Y, Liu Y. (2019) Neutrophil to lymphocyte ratio (NLR) as a prognostic marker for in-hospital mortality of patients with sepsis: A secondary analysis based on a single-center, retrospective, cohort study. Medicine (Baltimore). 98(46):e18029. Link
Patricio P, Paiva JA, Borrego LM. (2019) Immune Response in Bacterial and Candida Sepsis. Eur J Microbiol Immunol (Bp). 9(4):105-113. Link
Tang BM, Shojaei M, Teoh S, Meyers A, Ho J, Ball TB, Keynan Y, Pisipati A, Kumar A, Eisen DP, Lai K, Gillett M, Santram R, Geffers R, Schreiber J, Mozhui K, Huang S, Parnell GP, Nalos M, Holubova M, Chew T, Booth D, Kumar A, McLean A, Schughart K. (2019) Neutrophils-related host factors associated with severe disease and fatality in patients with influenza infection. Nat Commun. 31;10(1):3422. Link
Velavan TP, Meyer CG. (2020) Mild versus severe COVID-19: laboratory markers. Int J Infect Dis. 2020 Apr 25. pii: S1201-9712(20)30277-0. Link
Qin C, Zhou L, Hu Z, Zhang S, Yang S, Tao Y, Xie C, Ma K, Shang K, Wang W, Tian DS (2020) Dysregulation of immune response in patients with COVID-19 in Wuhan, China.Clin Infect Dis. 2020 Mar 12. pii: ciaa248 Link
Zuo Y, Yalavarthi S, Shi H, Gockman K, Zuo M, Madison JA, Blair CN, Weber A, Barnes BJ, Egeblad M, Woods RJ, Kanthi Y, Knight JS.(2020)Neutrophil extracellular traps in COVID-19. JCI Insight. 2020 Apr 24. pii: 138999 Link
This post is about some of the crazy stuff going on in trying to find better ways to treat Covid-19. Many of the treatments proposed to be encapsulated in this nanoparticles are already losing favor.
Laboratory Investigation of Effectiveness of Microencapsulated Biocontrol Antagonist Therapy and Immunogenicity Treatment for COVID-19 Virus
Alternate Title:
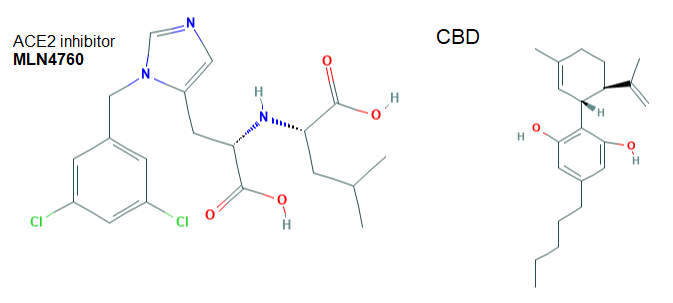
Investigation of Enhanced Experimental Nasal Muscosa Biocontrol Therapy and Immunogenicity Treatment for MERS, SARS, COV-2, (Corona-19), COVID-19 Viruses Using Nanoscopic Biopolymer/Biometal Micro-NanoCapsules With CuI Copper(I) iodide, Neocuproine Copper(II), Bathocuproine Disulfonic Acid Copper(I), Chloroquine, CBD and ACE-2 Inhibitors as Combined Functioning Antagonists
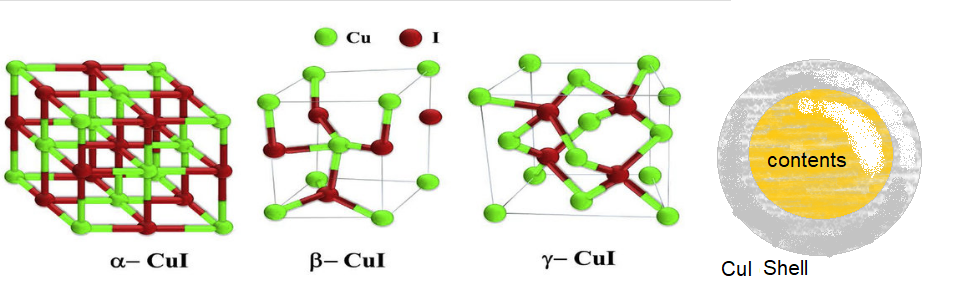
What is still not clear is if the core contents are actually part of the CuI matrix on the outside. Many of the proposed delivery drugs have nitrogens that may form complexes with cuprous and cupric copper. Many of the proposed contents are losing favor for the treatment of Covid-19.
Cuprous iodide forms polymers with a variety of phases. The Resnick group proposed have CBD a one of the materials in the core.
Medications used to treat parasitic infections
Melarsoprol is an acute toxin that is  under investigation in clinical trial NCT00330148 (Randomized Clinical Trial of Three Drug Combinations for Late-Stage Gambiense Human African Trypanosomiasis). This compound is very toxic to aquatic life with long lasting effects [Warning Hazardous to the aquatic environment, long-term hazard]  While melarsoprol is used to treat Trypanosoma brucei, the causative agent of sleeping sickness, it only worsens co-infections with human immunodeficiency virus (HIV). This drug stimulates the replication of several strains of HIV-1 in monocyte-derived DCs, and also renders such cells susceptible to HIV-2 infection.  We do not know how this drug will also increase the efficacy of the reverse transcription process in COVID-19 [1].
Melansoprol is a highly toxic arenite. Eflornithine is a suicide inhibitor of ornithine decarboxylase. The structure of ornithine is also shown. An arrow points to the carboxyl group that is removed.
Eflornithine is a difluoromethylated ornithine (DFMO) compound with antineoplastic activity. Eflornithine irreversibly inhibits ornithine decarboxylase, an enzyme required for polyamine biosynthesis, thereby inhibiting the formation and proliferation of tumor cells. DFMO has been shown to slow the replication of certain RNA viruses in a cell culture model [2].
Copper Chelators
Structures of neo- and bathocuproine from PubChem
Neocuproine is a chelator that has been used to treat copper overload in cultured cells. However the neocuproine MSDS (material safety data sheet) presents neocuproine as a highly toxic compound in the whole human. Neocuproine is toxic when inhaled or comes in contact with the skin. Its target organs are central nervous system, kidneys, liver, and optic nerve.
Bathocuproine is classified as an irritant by PubChem. While neocuproine-Cu+ was shown to inhibit the HIV-1 protease needed to cleave the viral poly-protein into individual proteins.[3]. However Neo-Cu+ failed to inhibit HIV-1 poly-protein processing in a T helper cell line. The authors proposed other methods of inhibition of viral replication. While Coivd-19 also has a viral protease needed to cleave the poly-protein, we have no evidence that inhibits the 3CL protease, or if it is possible to achieve inhibitory concentrations by spraying this material into the lungs. If nothing else, direct spraying into the lungs could limit the sites of side effects.
Forbes Recommended Covid-19 treatments
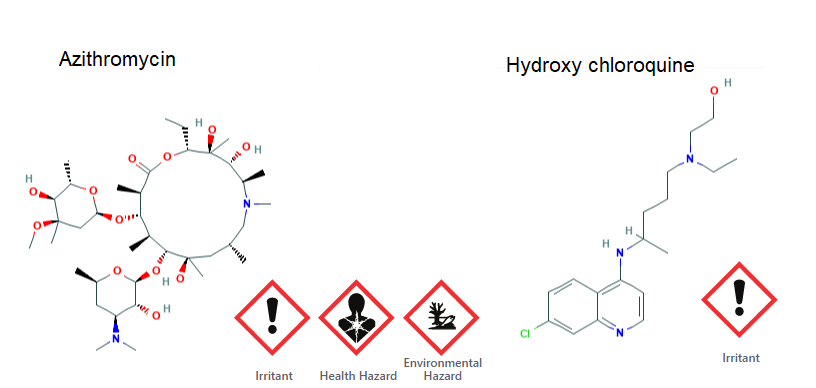
In April of this year hydroxychloroquine and azithromycin were touted by Forbes Magazine as a possible Covid-19 combination treatment.
Hydroxychloroquine is an anti-malarial that may also be an irritant at the wrong dosing and route of exposure.
Azythithromax is an antibiotic that inhibits bacterial protein synthesis by binding to the 50S ribosomal subunit of the bacterial 70S ribosome. PubChem reports rare cases of acute liver injury. Â
A French study published at the end of March followed the virologic and clinical outcomes of 11 consecutive patients hospitalized who received hydroxychloroquine (600 mg/d for 10 days) and azithromycin (500 mg day 1 and 250 mg days 2 to 5) using previously dosing [4]. No benefit of this combination treatment was observed. One patient had to discontinue treatment due to cardiac function abnormalities. a subsequent study of 200 Covid-19 patients on the combination therapy or dihyrochloroquine alone revealed a greater incidence in long QT abnormalities.  And just two days of this writing, ” These medications can pathologically prolong the QT interval and lead to malignant ventricular arrhythmias such that organized guidance on QT evaluation and management strategies are important to reduce morbidity associated with the potential large-scale use.” [6]
The ACE2 inhibitor and cannabidiol
ACCE2 counter blances ACE1 in terms of maintaining blood pressure [7]. ACE2 expression may be influeced by ACE1 inhibitors [7]. In addition to the lungs, ACE2 is expressed in the brain, gut, and kidney. The loss of ACE2 in the brain stem may facilitate an increase in sympathetic drive, alterations in the baroreflex, and exacerbation of hypertension.
And finally, there is some suggestion that CBD might make Covid-19 infections worse [8].
References
Barat C, Pepin J, Tremblay MJ. (2011) HIV-1 replication in monocyte-derived dendritic cells is stimulated by melarsoprol, one of the main drugs against human African trypanosomiasis. J Mol Biol. 2011 Jul 29;410(5):1052-64
Mounce BC, Cesaro T, Moratorio G, Hooikaas PJ, Yakovleva A, Werneke SW, Smith EC, Poirier EZ, Simon-Loriere E, Prot M, Tamietti C, Vitry S, Volle R, Khou C, Frenkiel MP, Sakuntabhai A, Delpeyroux F, Pardigon N, Flamand M, Barba-Spaeth G, Lafon M, Denison MR, Albert ML, Vignuzzi M. (2016)Inhibition of Polyamine Biosynthesis Is a Broad-Spectrum Strategy against RNA Viruses. J Virol. 2016 Oct 14;90(21):9683-9692. [PMC free article]
Davis DA, Branca AA, Pallenberg AJ, Marschner TM, Patt LM, Chatlynne LG, Humphrey RW, Yarchoan R, Levine RL. (1995)Inhibition of the human immunodeficiency virus-1 protease and human immunodeficiency virus-1 replication by bathocuproine disulfonic acid Cu1+. Arch Biochem Biophys. 322(1):127-34.
Molina JM, Delaugerre C, Le Goff J, Mela-Lima B, Ponscarme D, Goldwirt L, de Castro N.(2020)No evidence of rapid antiviral clearance or clinical benefit with the combination of hydroxychloroquine and azithromycin in patients with severe COVID-19 infection. Med Mal Infect. 2020 Jun;50(4):384. [PMC free article]
Saleh M, Gabriels J, Chang D, Kim BS, Mansoor A, Mahmood E, Makker P, Ismail H, Goldner B, Willner J, Beldner S, Mitra R, John R, Chinitz J, Skipitaris N, Mountantonakis S, Epstein LM.(2020 Apr 29) The Effect of Chloroquine, Hydroxychloroquine and Azithromycin on the Corrected QT Interval in Patients with SARS-CoV-2 Infection. Circ Arrhythm Electrophysiol.
Asensio E, Acunzo R, Uribe W, Saad EB, Sáenz LC.(2020) Recommendations for the measurement of the QT interval during the use of drugs for COVID-19 infection treatment. Updatable in accordance with the availability of new evidence. J Interv Card Electrophysiol. 2020 May 16
South AM, Diz DI, Chappell MC. (2020) COVID-19, ACE2, and the cardiovascular consequences. Am J Physiol Heart Circ Physiol. 2020 May 1;318(5):H1084-H1090. doi: 10.1152/ajpheart.00217.2020. Epub 2020 Mar 31.[PMC free article]Â [author pod cast]
Brown JD. (2020) Cannabidiol as prophylaxis for SARS-CoV-2 and COVID-19? Unfounded claims versus potential risks of medications during the pandemic.Res Social Adm Pharm. 2020 Mar 31. pii: S1551-7411(20)30300-4. [Cross Ref]
2023 update: This is another password protected post from May of 2020. We were actually forward thinking that maybe Covid-19 could be made worse by mycoplasma coinfections. A PubMed search on Mollicute and Coivd-19 reveals as much. Some day we should look at Cu(I)NA2 as an antibacterial for these cell wall lacking bacteria. In some ways this post to our founder who had this hunch.
Corona Viruses, Kawasaki’s Disease, and Children
Tang (2004) performed a PCR survey of pediatric cases of Kawasaki syndrome in Taiwan. RNA and DNA was extracted from throat swabs, and nasopharyngeal swabs. Nucleic acid sequences to identify the pathogens were amplified using PCR primers for enterovirus, adenovirus, influenza B, rhinovirus, metapneumovirus, and coronavirus. These authors found that children with Kawasaki’s syndrome were more likely to to have infections with common respiratory viruses [1].
Tables 3 and 5 are from ref [1]. The heart diagram is from an AHA site that has an excellent overview of Kawasaki’s syndrome and treatment.
COVID-19 and Mollicutes
Mollicutes is the new term for bacteria, formerly called mycoplasmas, that lack cell walls. Garth Nicolson, PhD and Gonzalo Ferreira de Mattos, MD, PhD and published a recent hypothesis paper proposing that COVID-19 deaths are due to coinfection with Mycoplasma pnuemoniae and related species of pathogenic bacteria [2].
Pneumonia is and inflammation of the aveoli of the lung that is generally caused by viral or bacterial infections. Fungi and parasites may also cause pneumonia.
CDC page on Mycoplasma pneumoniae is a good resource. Because these bacteria lack cell walls, therefore, β-lactam antibiotics, of which Penicillin is one, are of little use. Macrolides are commonly prescribed to children and adults with Mycoplasma infections. The CDC reports resistance as high as 90% in Asia with emerging cases of resistance in the United States and Europe. The CDC makes diagnosing Mollicute infections sound difficult and time consuming.
As a look back to 2016, Mycoplasma penumoniae was found in close to 14% of Kawasaki cases in the Children’s Hospital of Soochow University, China. These authors did not look for viral pathogens that were on the scene back in 2016. [4]
The CDC’s list of Mycoplasma pneumoniae Treatments
These antibiotics came from the CDC’s website with additional information of Wikipedia websites.
Macrolides (e.g., azithromycin): Children and adults Macrolides are generally considered the treatment of choice. However, clinicians should practice prudent use of macrolide drugs due to the emergence of macrolide-resistant strains of M. pneumoniae. Macrolides inhibit the translation of mRNA into proteins in bacteria.
Fluoroquinolones: Adults Fluoroquinolones inhibit DNA replication in bacteria. Unfortunately they have neurological side effects in humans.
Tetracyclines (e.g., doxycycline): Older children and adults Tetracyclines also inhibit the translation of mRNA into proteins in bacteria.
Clinicians should not prescribe fluoroquinolones and tetracyclines for young children under normal circumstances.
Concluding remarks
Mollicute and Covid-19 co-infections seem to be an emerging problem. Cases of Kawasaki Disease linked to mollicute and corona virus family infections raises some interesting questions. Could the right copper boost to the immune system prevent the use of antibiotics when bacterial co-infections are simply prolonging recovery?
References
Raha S, Mallick R, Basak S, Duttaroy AK.(2020) Is copper beneficial for COVID-19 patients? Med Hypotheses. 2020 May 5;142:109814. [PMC free article]
Chang LY, Lu CY, Shao PL, Lee PI, Lin MT, Fan TY, Cheng AL, Lee WL, Hu JJ, Yeh SJ, Chang CC, Chiang BL, Wu MH, Huang LM. (2014)Viral infections associated with Kawasaki disease. J Formos Med Assoc. 2014 Mar;113(3):148-54. [PMC free article]
Nicolson GL, Ferreira de Mattos G (2020) COVID-19 Coronavirus: Is Infection Along with Mycoplasma or other Bacteria Linked to Progression to a Lethal Outcome? International Journal of Clinical Medicine 11: [Cross Ref]
Tang Y, Yan W, Sun L, Huang J, Qian W, Hou M, Lv H.(2016) Kawasaki disease associated with Mycoplasma pneumoniae. Ital J Pediatr. 42(1):83 [PMC free article]