The importance of copper in the function of neutrophils and lymphocytes as been addressed on another post. This post never actually presented real data. We retrospectively analyzed data from a study performed by KGK Synergize in 2014. KGK analyzed the raw numbers of neutrophils and lymphocytes using an ANOVA model because the data were nonparametric. This post presents how we analyzed data collected by our CRO that has be registered at https://clinicaltrials.gov/ct2/show/NCT04737278. The graphs sort of tell their own story. Until FDA gives the green light, we are making no medical claims.
This free stats site uses six different sets for normality: Shapiro-Wilk, Shapiro-Francia, D’Agostino-Pearson, Jarque-Bera, Cramer-von Mises, Anderson-Darling. The sensitivity was set at p<0.05.
Given these results, it was decided to skip the ANCOVA in favor of ANOVA since the assumption of normality is met for NLR data. Went back and checked the neutrophil counts. Very definitely not a normal distribution.
| Placebo1 | Placebo2 | Placebo3 | Cu 1 | Cu2 | Cu3 | |
| Minimum | 1.142857 | 0.958333 | 1 | 0.619048 | 0.625 | 0.766667 |
| Maximum | 3.727273 | 4.1 | 5 | 4.666667 | 4.6 | 3.833333 |
| Sum | 55.58982 | 53.29325 | 61.52245 | 49.65535 | 49.66772 | 45.39949 |
| Points | 28 | 28 | 28 | 28 | 28 | 28 |
| Mean | 1.985351 | 1.90333 | 2.19723 | 1.773405 | 1.773847 | 1.62141 |
| Median | 1.757143 | 1.745098 | 2.041667 | 1.666667 | 1.75 | 1.439103 |
| RMS | 2.091988 | 2.016828 | 2.410644 | 1.961878 | 1.927315 | 1.758534 |
| Std Deviation | 0.67149 | 0.679269 | 1.009854 | 0.854442 | 0.767495 | 0.693279 |
| Variance | 0.450899 | 0.461407 | 1.019805 | 0.730072 | 0.589048 | 0.480636 |
| Std Error | 0.1269 | 0.12837 | 0.190844 | 0.161474 | 0.145043 | 0.131017 |
| Skewness | 1.284053 | 1.271123 | 1.440843 | 1.756352 | 1.641878 | 1.399153 |
| Kurtosis | 0.920368 | 1.987952 | 1.794157 | 3.631511 | 4.685251 | 2.016536 |
| normality | Pass all | Pass 1st 4 | Pass all | Pass all | Pass all | Pass all |
Having proven normal distribution another free stats website was used to perform ANOVA. A free site was used for 2-way ANOVA.
| ANOVA Summary | |||||
| Source | SS | df | MS | F | p |
| visits | 0.41 | 1 | 0.41 | 0.65 | 0.422 |
| treatments | 3.26 | 1 | 3.26 | 5.14 | 0.025 |
| visits x treatments | 1.31 | 1 | 1.31 | 2.07 | 0.153 |
| Error | 66.57 | 105 | 0.63 | ||
| Total | 71.55 | 108 |
| Placebo | Cu(I)NA2 | P Value | |
| Mean ± SD (N) Median (Min – Max) | Mean ± SD (N) Median (Min – Max) | ||
| Neutrophils (109/L) | |||
| Screening | 3.49 ± 1.12 (28) 3.4 (1.8 – 6.4) | 3.45 ± 1.16 (28) 3.2 (1.3 – 6.3) | – |
| Baseline | 3.35 ± 1.13 (28) 3.1 (1.5 – 6.2) | 3.28 ± 1.06 (28) 3.15 (1 – 6) | – |
| Visit 3 (Day 28) | 3.60 ± 1.13 (27) 3.6 (1.7 – 6.4) | 3.15 ± 1.19 (26) 2.85 (1.5 – 7.2) | 0.03* |
| Change from Baseline to Visit 3 | 0.32 ± 0.83 (27) 0.2 (-0.8 – 3.6) p = 0.05§ | -0.13 ± 0.73 (26) 0.05 (-1.9 – 1.2) p = 0.38§ | – |
| Lymphocytes (109/L) | |||
| Screening | 1.84 ± 0.51 (28) 1.9 (0.8 – 2.8) | 2.15 ± 0.69 (28) 2.15 (0.6 – 3.4) | – |
| Baseline | 1.83 ± 0.51 (28) 1.8 (0.9 – 2.7) | 2.01 ± 0.64 (28) 1.9 (0.5 – 3.2) | – |
| Visit 3 (Day 28) | 1.74 ± 0.51 (27) 1.8 (0.9 – 2.6) | 2.04 ± 0.72 (26) 2 (0.6 – 3.4) | <0.01* |
| Change from Baseline to Visit 3 | -0.08 ± 0.34 (27) 0 (-0.8 – 0.4) p = 0.22§ | 0.03 ± 0.39 (26) 0.1 (-0.8 – 1) p = 0.73§ | – |
| Neutrophil to lymphocyte ratio | |||
| Screening | 1.99 ± 0.67 1.76 (1.14-3.72) | 1.77 ± 0.85 1.67 (0.62-4.57) | |
| Baseline | 1.90 ± 0.68 1.75 (0.96-4.1) | 1.77± 0.77 1.75 (0.625-4.6) | p=0.44§ |
| Visit 3 (Day 28) | 2.20 ± 1.03 2.08 (1.0-5.0) p=0.066§ | 1.62 ± 0.69 1.44 (0.77-3.83) p=0.054§ | p=0.03∆ |
| Change from Baseline to Visit 3 | -0.294 ± 0.813 -0.049 -3.38 to 1.38 | 0.152 ± 0.400 0.123 -0.625 to 0.902 | p<0.05§ |
Note that a change in baseline to Visit 3 is the baseline value minus the Visit 3 value. A The mean change in baseline to visit 3 decreased in the placebo group meaning that the NLR increased in the placebo group.
Examples of Cu(I)NA2 helping those that are..
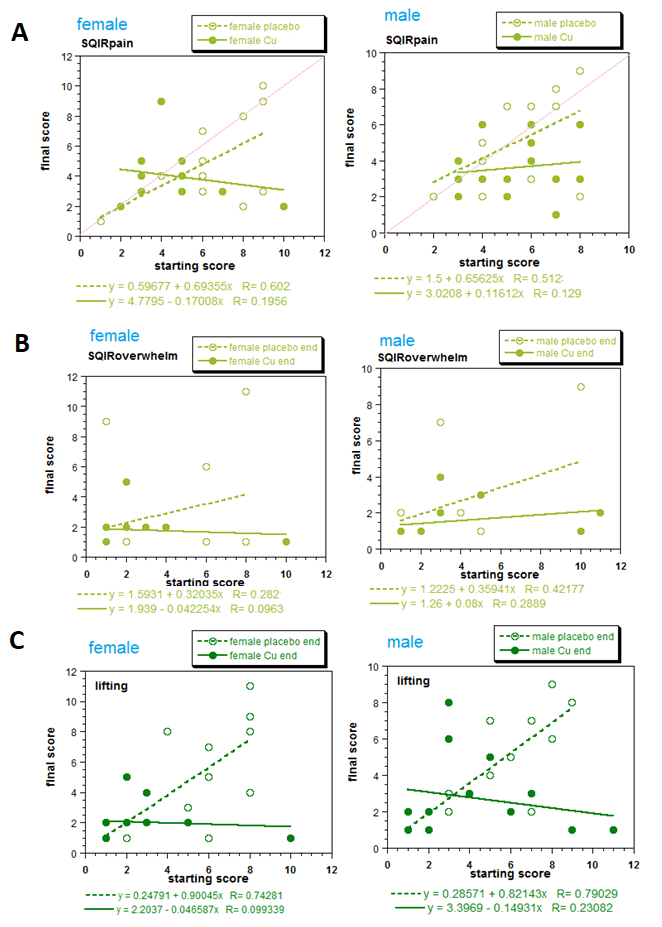
Mitosynergy has a conviction that customers that are worse off have the most symptom improvement. This multiple regression model provides preliminary statistical backing for this conviction. The red line of “manuscript in preparation Figure 4A illustrates what one would see if there was no improvement of the baseline score on the X-axis to the score on day 28 on the Y-axis. The slope would be 1.0. The equation of a line documenting a complete “cure” would have a slope of 0 and and a Y-intercept of 0 to 1. The placebo slopes were about 0.65, close enough to 1.0. The slopes of theCu(I)NA2 line for the females was less than 0, -0.17. Examination of the NLR will reveal a different phenomenon.
A graphical view of the NLR
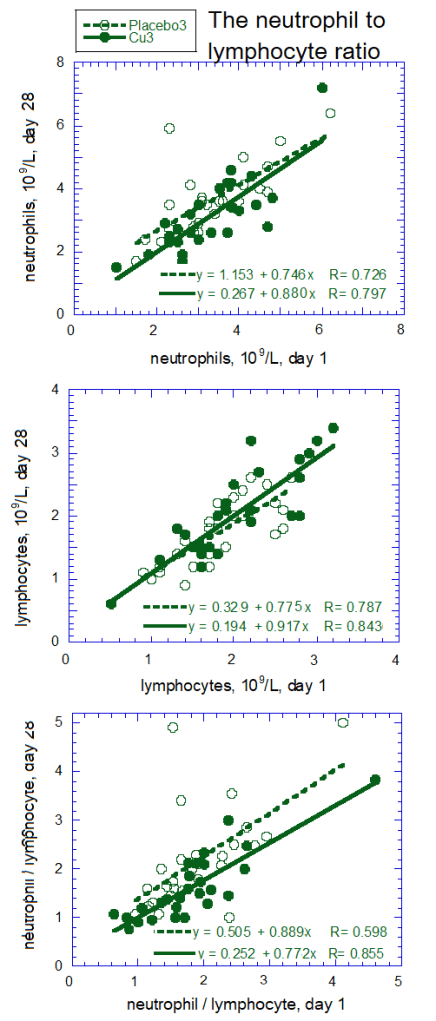
Figure 5 Neutrophils, lymphocytes, and the neutrophil /lymphocyte ratios: the amount on day 28 as a function of baseline, day 1.
Male and female data were combined when analyzing neutrophil and lymphocyte counts because separating the data did not reveal any difference. Population variations are very apparent when the data are presented graphically. The interesting phenomenon is that the slopes of the lines of the placebo and Cu(I)NA2 were statistically the same. The y-intercepts appear to be different. While these small studies are to be interpreted with caution, Cu(I)NA2 seems to improve the NLR ratio for all the participants a little.