This post was initiated as an effort to better understand a previous post showing association of CD8 cytotoxic T cell surface proteins PD-1 and Tim-3 with Long Covid. A 2010 study documented coregulation of CD8 T cell exhaustion by Tim-3 and PD-1 during chronic lymphocytic choriomeningitis virus infection (LCM) [1] Could Long Coivd be a chronic infection enabled by exhausted T cells? PD-1/Tim-3 play a role in T cell exhaustion in cancer. A study has used H2 gas to bolster the mitochondria in human cancer patients. [2] Cuprous niacin could have an even greater potential as an immunomodulator for more than just Long Covid! For now, Long Covid is where the FDA interest seems to be. This study [1] tells us that anti viral CD8+ T cell surface receptors PD-1 and Tim-3 are something we should include in the clinical trial. Ref [2] that PD-1 has a strong mitochondrial and NAD+ connection. PD-1
During chronic viral infections such as HIV, hepatitis B virus, and hepatitis C virus
(HCV) , CD8 T cells become “exhausted†as characterized by [1]
- Inability to produce cytokines
- Inability to lyse virus infected cells
- Inability to proliferate
Materials and Methods [1]
- Six-week-old female C57BL/6 mice were were intraperitoneally
infected with 2 × 105 pfu of LCMV - Lymphocytes were isolated from tissue including spleen, liver, lung, and blood as previously described.
- To detect degranulation, splenocytes were stimulated with individual LCMV peptides or a pool of eight LCMV epitopes for 5 h in the presence of brefeldin, monensin, anti–CD107a-FITC, and anti–CD107b-FITC. Cells were then analyzed on by flow cytometry to determine surface markers.
- CD8 T cells were purified to more than 90% purity using magnetic beads.
- Tim3+PD1+ and Tim3-PD1+ CD8 T and cocultured with splenocytes from Thy1.1+ C57BL/6 mice in the presence of LCMV peptides for 3 d. Proliferation was measured suing flow cytometry.
- For blockade of PD-1 pathway, 200 μg of rat antimouse PD-L1 antibody were administered intraperitoneally every 3 d for 2 wk.
- For blockade of Tim-3 pathway, 100 μg of Tim-3-Ig fusion protein were injected intraperitoneally every 2 d for 2 wk.
- Titers of virus from serum or homogenized tissue sample were determined by plaque assay on Vero cells.
Fig 1 Intro to flow cytometry and acute vs chronic viral infections
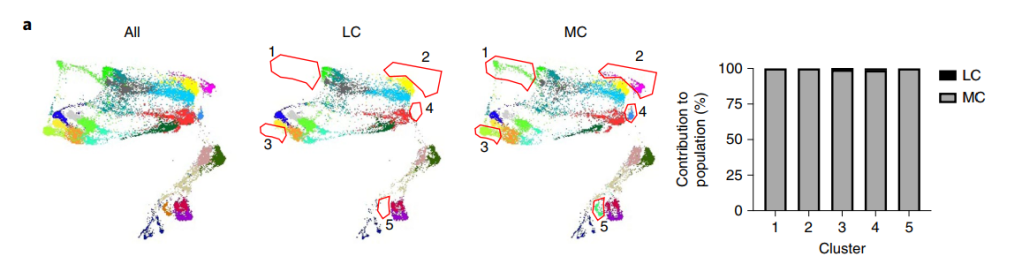
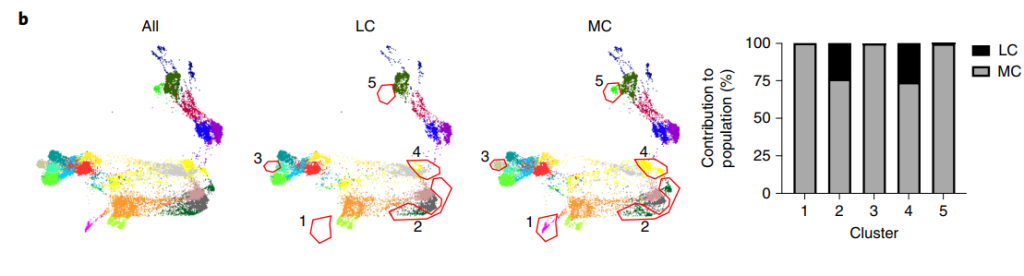
Figure 1 Panels B and D showed flow cytometry quadrant plots for all data points. [1] The antibodies that recognize the surface markers are conjugated with different colored fluorescent tags. Cells that are negative for both surface marker are in the lower left quadrant. Those that are positive for both, in this case GP33 and Tim3 appear in the upper right quadrant. Panel 1A is a series of histogram plots. The X-axis is bins of signal intensity for the CD33 antibody. The Y-axis is the counts, or number of cells with a given signal intensity. GP33 appears to be a LCMV peptide. These T cells in acute and/or chronic infections should recognize peptides from the surface of LCMV.
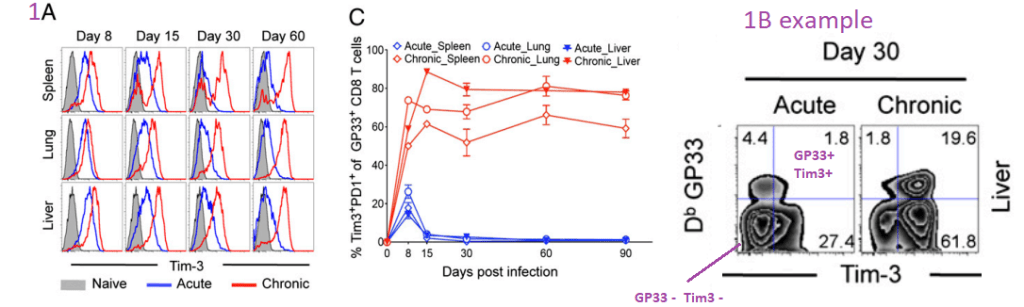
Of all of the T tells that have receptors that bind to GP33, the majority also express Tim3 and PD1 receptors in chronic, but not acute infections.
Fig. 2 Co-expression of Tim-3 and PD-1 correlates with …
more severe exhaustion of LCMV-specific CD8 T cells during chronic infection. Functions of
Tim3+PD1+ or Tim3-PD1+ CD8 T cells were analyzed using splenocytes at day 50 after infection. [1]
(A) This post is omitting panel on that demonstrates the isolation protocol.
(B) Frequency of GP33- or GP276-specific CD8 T cells producing cytokine after
stimulation for 5 h with GP33-41 or GP276-286 peptides.  These cytokines seem to be in secretory granules or something. Their synthesis and/or secretion is dependent on binding of peptides from the LCMV to the T cell receptors. These panels examine the ratio of cells expressing producing cytokines to those T cells with receptors receptors that recognize LCMV peptides. Having Tim3 and PD1 on the cell surface tends to correlate with low inflammatory cytokine
(C) Frequency of Tim3+PD1+, Tim3-PD1+, or Tim3-PD1- CD8 T cells producing IL-10 was analyzed after stimulation for 5 h with the LCMV peptide. Data are representative of three independent experiments. Error bars represent SEM. LCMV pool consists of GP33-41, GP276-2. Note the lavender arrow that emphasizes the Tim3 negative status of the empty circles. These T cells do not produce the inhibitory cytokine IL10.
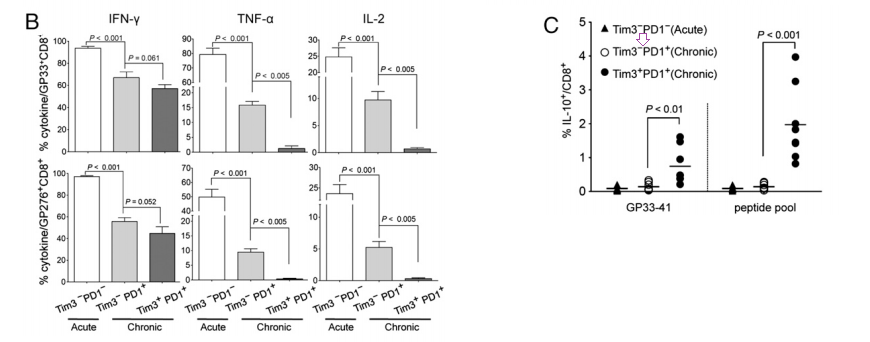
Fig. 3. In vivo blockade of Tim-3 and PD-1 pathways…
enhances virus-specific CD8 T-cell responses during chronic viral infection. [1]
Chronically infected C57BL/6 mice (80 d after infection) were treated every third day or every eeks other day for 2 wk with αPDL1 or Tim3Ig, respectively. Frequency of GP33-specific CD8 T cells before and after treatment of individual mouse is shown in the blood. Total number of GP33-specific CD8 T cells in the indicated
tissues at 2 wk after treatment. Data are representative of three independent experiments with five to six mice per group in each experiment
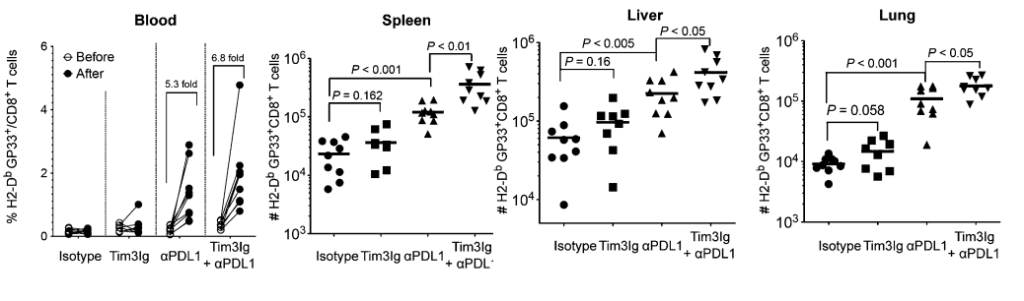
In the three tissues but not the blood, just knocking down PDL1 increases the proportion of all CD8+ cytotoxic T cells that express the GP33+ receptors that recognize the LCMV peptides.
Fig. 4. Dual blockade of Tim-3 and PD-1 pathways…
enhances function in exhausted virus-specific CD8 T cells. [1]
(A) IFN-γ production and degranulation by CD8 T cells in treated mice at 2 wk after therapy. The percentage of IFN-γ+CD107+ CD8 T cells specific for each of the LCMV peptides are summarized.
(B) Polyfunctional (TNF-α+IFN-γ+) CD8 T cells in treated mice at 2 wk after therapy.
(C) The proliferation of antigen specific CD8 T cell after dual blockade is shown as the percentage of Ki67+ on LCMV GP33-specific CD8 T cells. Data are representative of three independent experiments with five to six mice per group in each experiment.
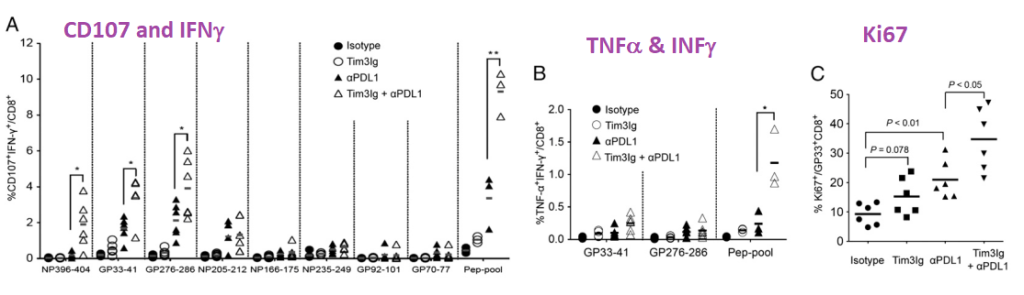
While it takes the peptide pool to really get the T cells to crank out TNFα and INFγ, just peptides restricted to smaller regions of LCMV are effective in increasing T cell proliferation as measured by Ki67.
Fig. 5. Dual blockade of Tim-3 and PD-1 pathways…
enhances viral control. [1]
Viral titer was determined by plaque assay in the blood before and after treatment. Viral load in spleen, liver, and lung at 2 wk after treatment is shown. Data are representative of three independent experiments with five to six mice per group in each experiment. Error bars represent standard error of the means.
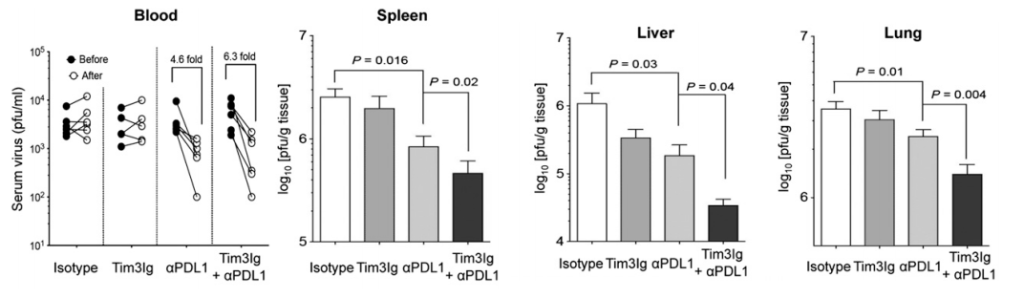
Never mind the decreased proliferation and cytokine production by exhausted CD8+ T cells, inhibiting PD-1 and Tim-3 reduces the LCMV viral load in this mouse study. What if Long Covid really is a chronic infection that escapes the immune system? This site has covered the role of copper deficiency in T cell exhaustion. What if bolstering the mitochondria can prevent PD-1 from being expressed in the first place?
It should also be noted that the PD1/PD-L1/Tim3 system plays a role in cancer and tuberculosis infections as well as transplanted organ tolerance and autoimmunity. [2] The Wolf review did not mention chronic Lyme Disease infections. These authors did go into the many ligands of Tim3 and the possible benefits of Tim3 ligand binding blockage.
And on to the mitochondria [3]
This story [1] is all very interesting, but what is the connection to the mitochondria? This question was addressed by a human study of cancer patients with colorectal carcinoma on the PD1 antibody chemotherapy agent Nivolumab. [2] Specifically, these patients had issues with CD8+ T cells that also expressed PD-1 and Tim3. [3] Akagi and Baba covered many important points as to why they thought there was mitochondrial dysfunction and that the patients would benefit form H2 gas therapy.
- Nivolumab cure rate of 20‑30% and needs a biomarker to distinguish responders from non-responders. ,
- These T cell dysfunctions of exhausted T cells are inversely correlated with decreased
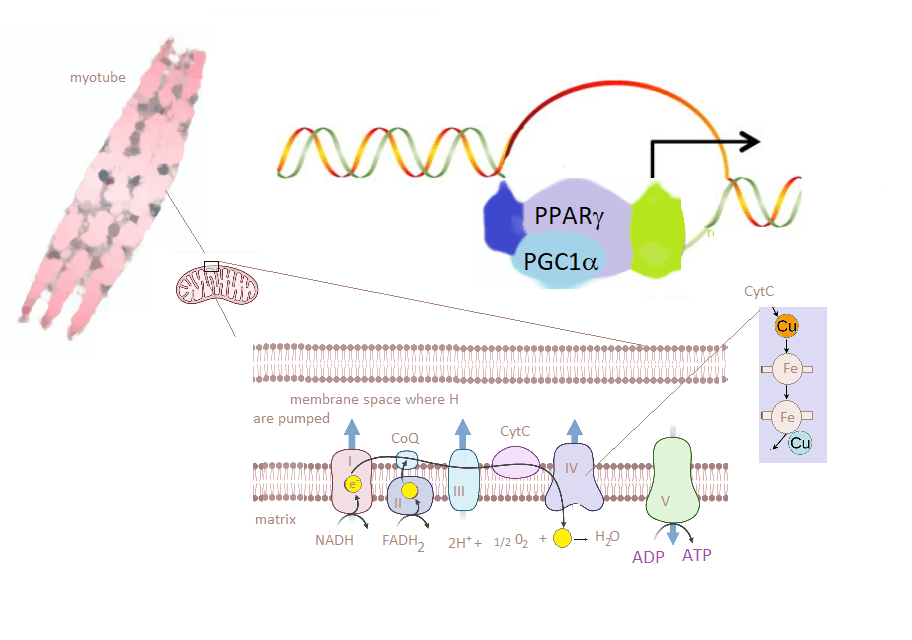
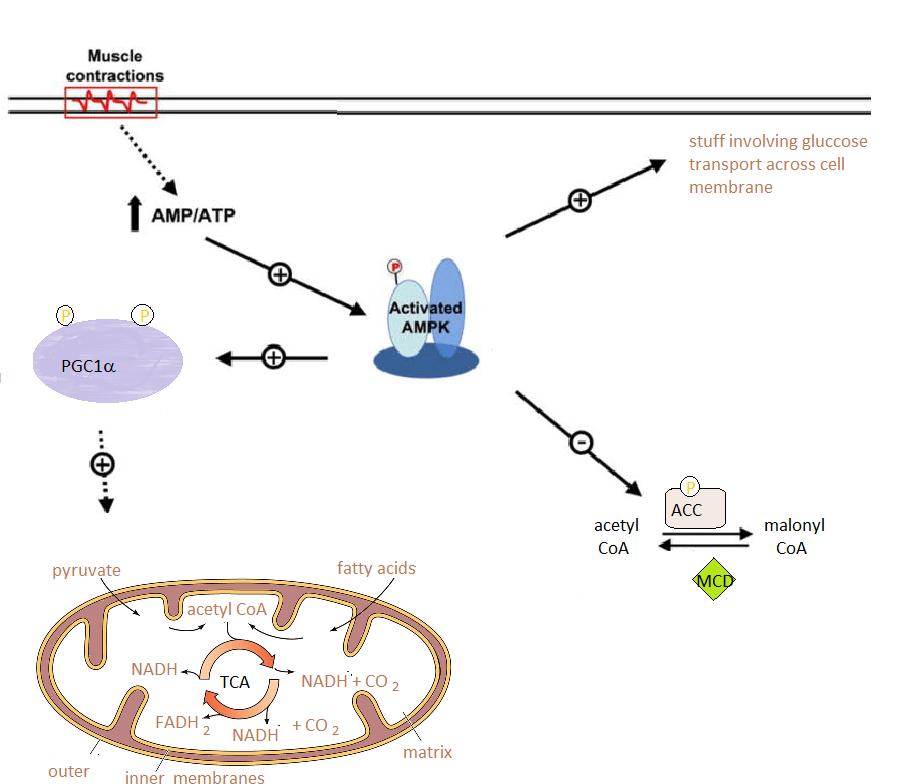
mitochondrial function (3), - which is caused by progressive loss of peroxisome proliferator‑activated receptor‑γ coactivator 1α (PGC1α), a regulator of mitochondrial replication that is controlled by a variety of signaling pathways
- (Akt, p38‑MARK, AMPK, SIRT1, PRMT1… Note that AMPK and SIRT1 pathways are connected with NAD+, ADP/ATP, and overall mitochondrial function.
- The authors reported that the proportion of PD‑1+terminal CD8+ T cells containing PDT+ and PDT‑ (exhausted CD8+T cells) in the peripheral blood of colorectal cancer patients was reduced by hydrogen gas, an activator of PGC1‑α,
- They used serum coenzyme Q as a marker of mitochondrial function. CoQ10 was in the serum was highly associated with patient prognosis. [2]
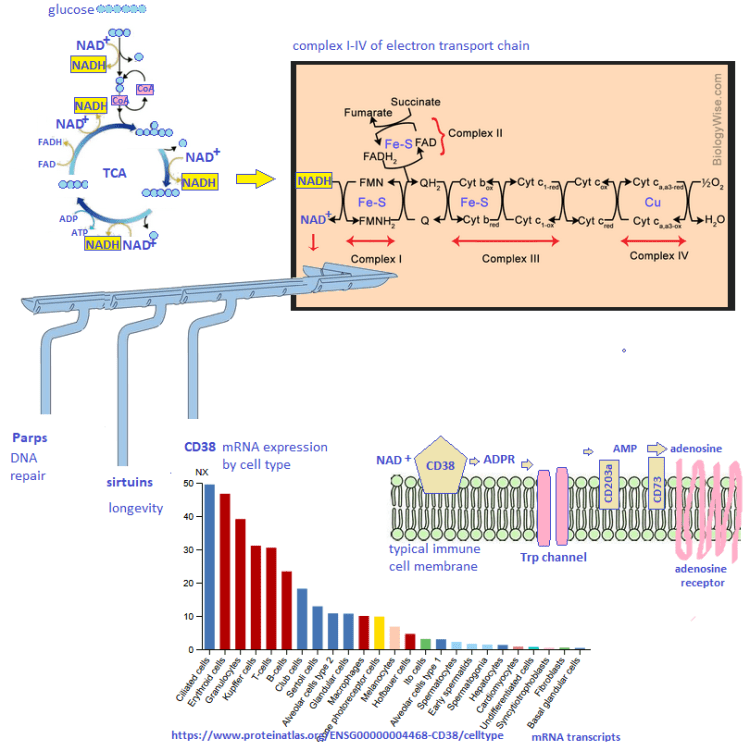
The authors found that some patients responded to hydrogen gas and that others did not. The PD1/Tim3 + T cells (PDT+) decreased with the H2 therapy. PDT+ was inversely correlated with serum CoQ10. The authors claimed no appropriate method to easily measure mitochondrial function. They argued that CoQ10 is part of the electron transport chain. If so, what is it doing in the serum? The Seahorse respirometer is a not so easy way to measure cellular respiration as is cellular ATP content. Akagi and Baba discussed NAD+ pathways and gene transcription. They also discussed the putative role of H2 in turning components of NAD+ and ADP/ATP ration gene transcription. So H2 has some benefit. It does not address the possibility that the antiviral cytotoxic T cell does not have enough nutrients to do its duty so it is expressing PD-1 so that it may be turned off.
Aging
Onorati 2022 introduced the concept that the senescent associated secretory phenotype (SASP) upregulates PD-L1 expression.

The Tchkonia review [4] discussed signaling pathways like p53/p21..
Triggers may include DNA damage, reactive oxygen species, and protein aggregation. They introduced an interesting concept of “sterile inflammation” as opposed to inflammation that results from a pathogen infection.
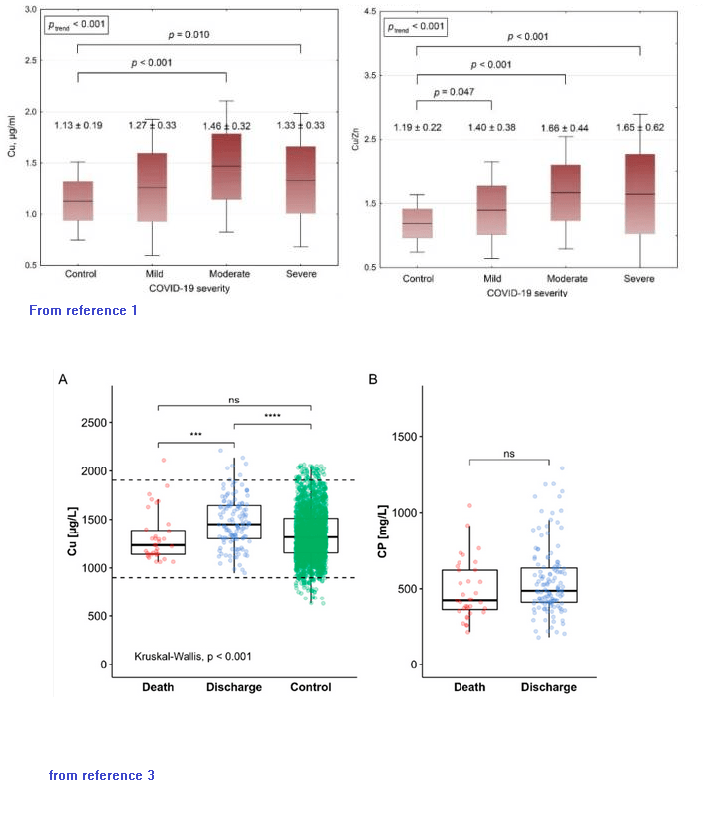
The role of copper deficiency and mitochondria dysfunction was not discussed, but we think this may be relevant in aging. . The role of Cu/Zn superoxide dismutase was also not discussed in terms of reactive oxygen species.
- PD-L1 was increased in human diploid lung fibroblasts induced to undergo senescence.
- This induction requires the SASP
- The SASP “fires” through second messenger protein kinases called JAK-STAT
- mTOR, the nutrient sensing master regulator, is involved.
- PD-L1 is upregulated in interstitial lung disease.
References
- Jin, H. T., Anderson, A. C., Tan, W. G., West, E. E., Ha, S. J., Araki, K., Freeman, G. J., Kuchroo, V. K., & Ahmed, R. (2010). Cooperation of Tim-3 and PD-1 in CD8 T-cell exhaustion during chronic viral infection. Proceedings of the National Academy of Sciences of the United States of America, 107(33), 14733–14738. PMC free article
- Wolf Y, Anderson AC, Kuchroo VK. TIM3 comes of age as an inhibitory receptor. Nat Rev Immunol. 2020 Mar;20(3):173-185. PMC free article
- Akagi J, Baba H. Hydrogen gas activates coenzyme Q10 to restore exhausted CD8+ T cells, especially PD-1+Tim3+terminal CD8+ T cells, leading to better nivolumab outcomes in patients with lung cancer. Oncol Lett. 2020 Nov;20(5):258 PMC free article
- Onorati A, Havas AP, Lin B, Rajagopal J, Sen P, Adams PD, Dou Z. Upregulation of PD-L1 in Senescence and Aging. Mol Cell Biol. 2022 Oct 20;42(10):e0017122. PMC free article
- Tchkonia T, Zhu Y, van Deursen J, Campisi J, Kirkland JL. Cellular senescence and the senescent secretory phenotype: therapeutic opportunities. J Clin Invest. 2013 Mar;123(3):966-72. PMC free article